Your genetic code holds valuable information about cardiovascular wellness, particularly regarding how your body processes and transports fats and cholesterol through the bloodstream. Understanding lipoprotein genetic health risj factors empowers individuals to take proactive steps toward heart health management, especially when family history suggests elevated risks. Modern lab testing makes it easier than ever to identify these inherited vulnerabilities and develop personalized prevention strategies.
Big picture
- Lipoproteins are genetic fat carriers that transport cholesterol and triglycerides throughout your body, and variations in the genes controlling them can significantly increase cardiovascular disease risk
- Inherited conditions like elevated Lp(a) affect approximately 20% of the global population and represent one of the strongest genetic risk factors for heart attack and stroke
- Early detection through lab testing enables intervention before symptoms appear, particularly important for those with family histories of premature heart disease
- Direct-access testing services allow you to order labs without a doctor visit, making cardiovascular genetic screening more accessible and affordable
- Knowing your genetic risk helps you and your healthcare team develop targeted prevention strategies including lifestyle modifications and potential pharmaceutical interventions
Understanding Lipoprotein Genetic Variations
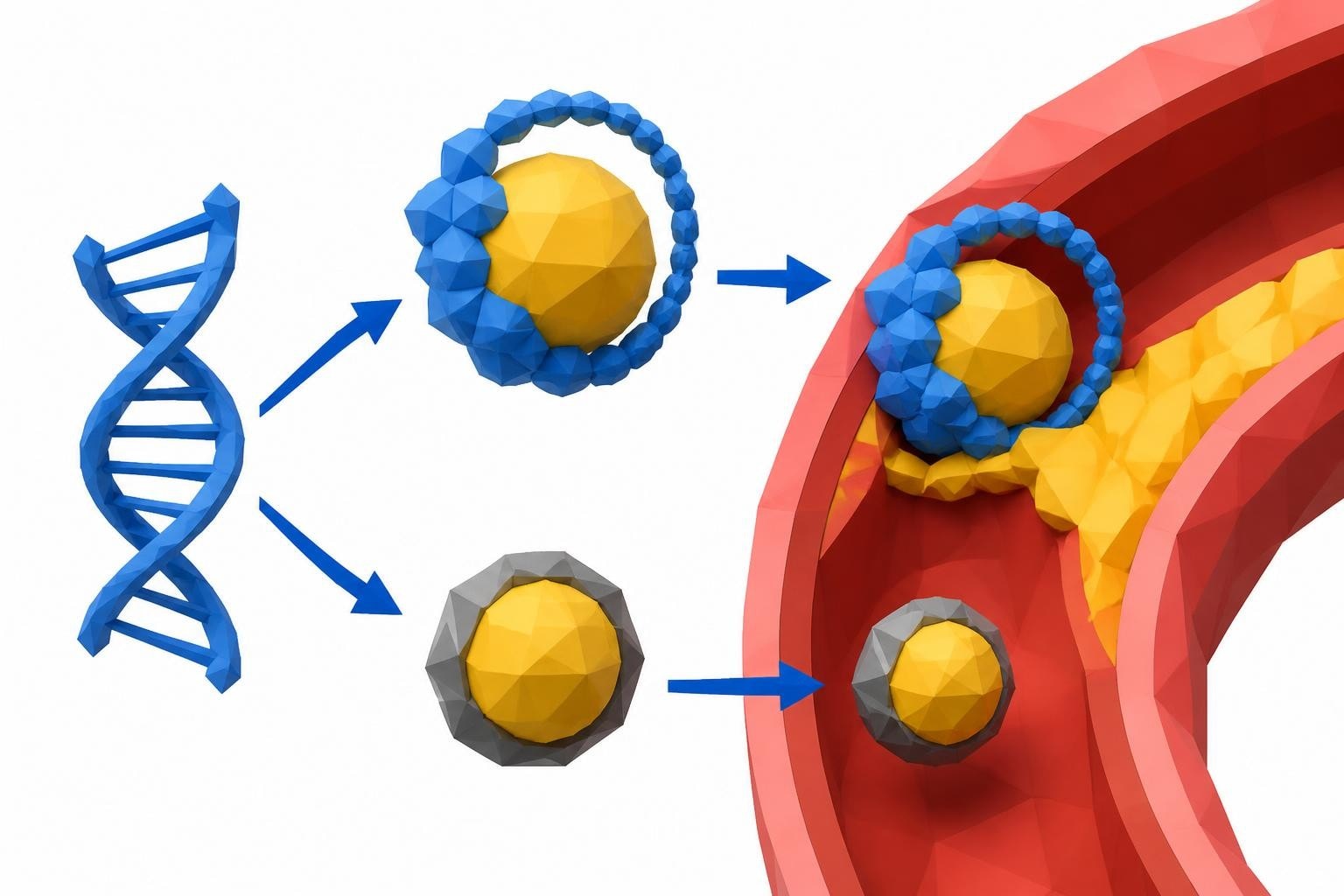
Lipoproteins function as transport vehicles, carrying fats and cholesterol that cannot dissolve in blood on their own. These complex particles consist of proteins called apolipoproteins surrounding a core of lipids. Your genetic blueprint determines how efficiently your body produces, processes, and clears these particles from circulation.
The Role of Key Genes
Several genes play critical roles in lipoprotein metabolism. The APOB gene produces apolipoprotein B, a primary structural component of low-density lipoprotein (LDL) cholesterol particles. Mutations in this gene can lead to familial hypercholesterolemia, causing dramatically elevated cholesterol levels from birth. Similarly, the LPL gene encodes lipoprotein lipase, an enzyme responsible for breaking down triglyceride-rich lipoproteins. Deficiencies in this enzyme can result in severe hypertriglyceridemia.
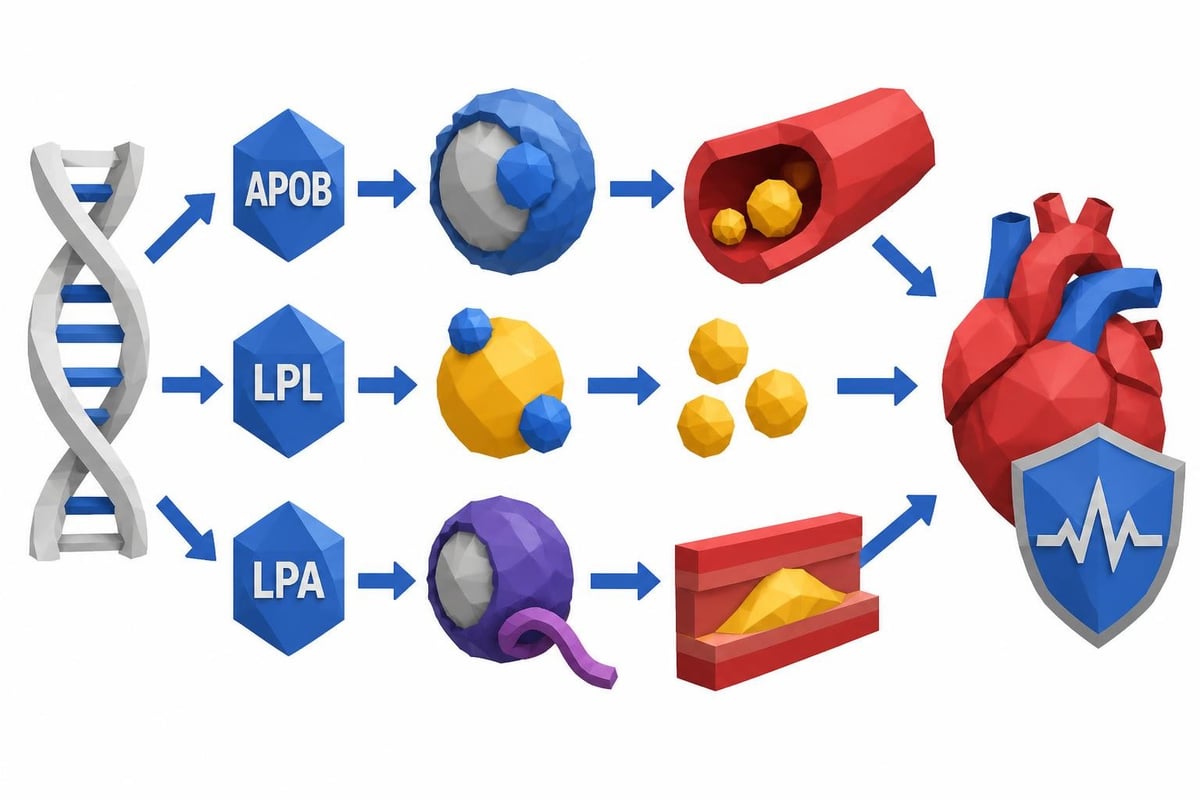
When examining lipoprotein genetic health risj profiles, the LPA gene deserves special attention. This gene controls production of lipoprotein(a), abbreviated as Lp(a), a particle similar to LDL but with an additional protein component called apolipoprotein(a). Unlike standard cholesterol levels that respond to diet and exercise, Lp(a) levels are primarily determined by genetics and remain relatively stable throughout life.
Familial Hypercholesterolemia
This inherited disorder represents one of the most common genetic conditions affecting lipoprotein metabolism, occurring in approximately 1 in 250 people. Individuals with familial hypercholesterolemia cannot effectively remove LDL cholesterol from their bloodstream, leading to extremely high cholesterol levels even with healthy lifestyle habits.
The condition follows an autosomal dominant inheritance pattern, meaning just one defective gene copy from either parent causes the disorder. Children of affected individuals have a 50% chance of inheriting the condition. Without treatment, men with familial hypercholesterolemia typically develop heart disease in their 40s or 50s, while women often experience cardiovascular events in their 50s or 60s.
Lipoprotein(a): The Hidden Genetic Risk Factor
Among lipoprotein genetic health risj factors, elevated Lp(a) stands out for several reasons. This particle promotes atherosclerosis through multiple mechanisms, including enhanced LDL deposition in arterial walls, increased inflammation, and interference with normal blood clot dissolution. Recent research has established Lp(a) as an independent and causal risk factor for cardiovascular disease.
| Lipoprotein(a) Risk Levels | mg/dL Range | Cardiovascular Impact |
|---|---|---|
| Desirable | < 30 | Minimal genetic risk |
| Borderline | 30-50 | Moderately elevated risk |
| High | 50-100 | Significantly elevated risk |
| Very High | > 100 | Severely elevated risk requiring aggressive management |
Why Lp(a) Testing Matters
The CDC emphasizes that Lp(a) is genetically inherited and associated with increased risks for heart attack, stroke, and aortic stenosis. Despite its significance, Lp(a) testing remains underutilized in clinical practice. Many individuals discover elevated levels only after experiencing a cardiovascular event or when pursuing comprehensive heart health screening.
Harvard Health highlights that Lp(a) represents an inherited cause of early heart disease, making testing particularly valuable for:
- Individuals with family histories of premature cardiovascular disease
- People who have experienced heart attacks or strokes despite normal cholesterol levels
- Those with recurrent cardiovascular events despite optimal medical therapy
- Anyone with a family member diagnosed with elevated Lp(a)
Because Lp(a) levels remain stable throughout adulthood, testing once provides lifelong information about this genetic risk factor.
Identifying Your Genetic Lipoprotein Profile
Recommended Panel
Advanced Heart Health Panel
Save $6Go beyond basic cholesterol testing. This advanced panel includes the markers cardiologists use to assess true cardiovascular risk: ApoB, Lp(a), homocysteine, and inflammation.
Includes 10 biomarkers
$86
Fasting required
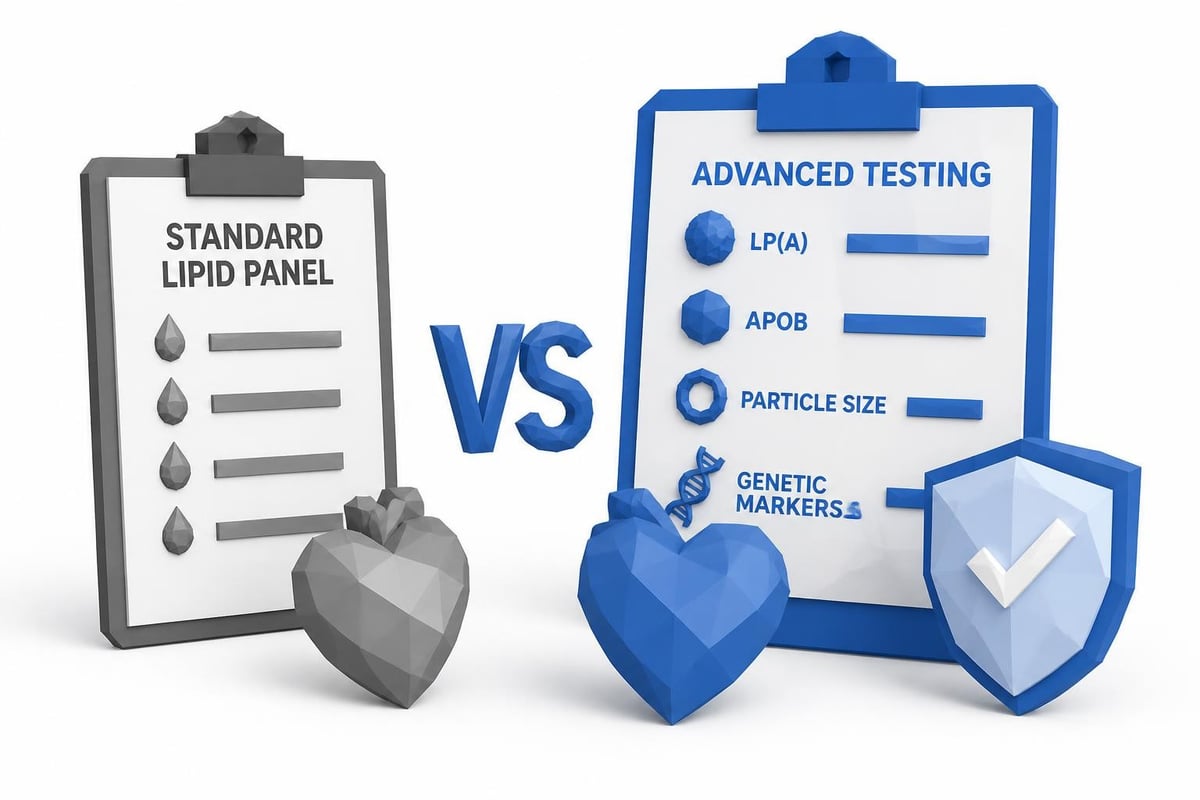
Assessing lipoprotein genetic health risj begins with comprehensive lipid testing that extends beyond basic cholesterol panels. Standard lipid panels measure total cholesterol, LDL, HDL, and triglycerides but miss critical genetic markers like Lp(a) and advanced cholesterol subfractions.
Components of Advanced Lipoprotein Testing
Lipoprotein(a) measurement provides the single most important genetic lipid marker. Since levels are genetically determined, one test offers permanent risk assessment. Results help determine whether aggressive cholesterol management strategies are warranted even when standard cholesterol numbers appear acceptable.
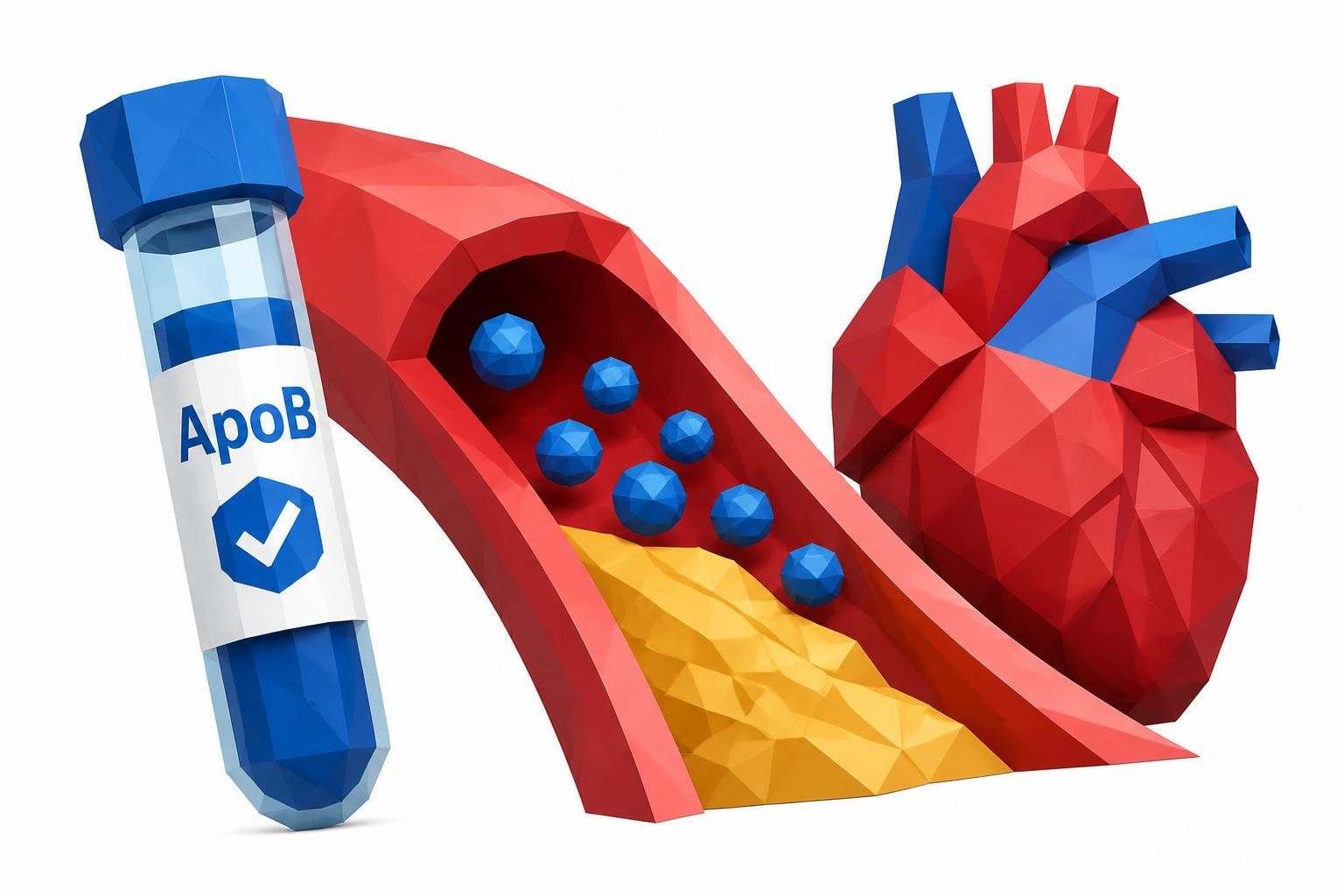
Apolipoprotein B (ApoB) quantification counts the actual number of atherogenic particles in circulation, providing more accurate cardiovascular risk assessment than LDL cholesterol alone. Each LDL particle contains one ApoB molecule, making this measurement a direct particle count rather than an estimate of cholesterol content.
Advanced lipid panels may include particle size analysis, distinguishing between large, fluffy LDL particles and small, dense ones that more readily penetrate arterial walls. This information reveals inherited patterns of lipoprotein composition affecting cardiovascular risk.
Accessible testing options have expanded significantly. Services allowing you to access affordable lab testing without insurance barriers make comprehensive lipoprotein screening available to more people. Understanding lab test pricing upfront eliminates surprises and enables proactive health management.
Genetic Testing for Lipoprotein Disorders
For individuals with strong family histories or clinical presentations suggesting inherited lipoprotein disorders, genetic testing identifies specific mutations. Panel testing can evaluate multiple genes simultaneously, including those affecting LDL receptor function, ApoB structure, and PCSK9 enzyme activity.
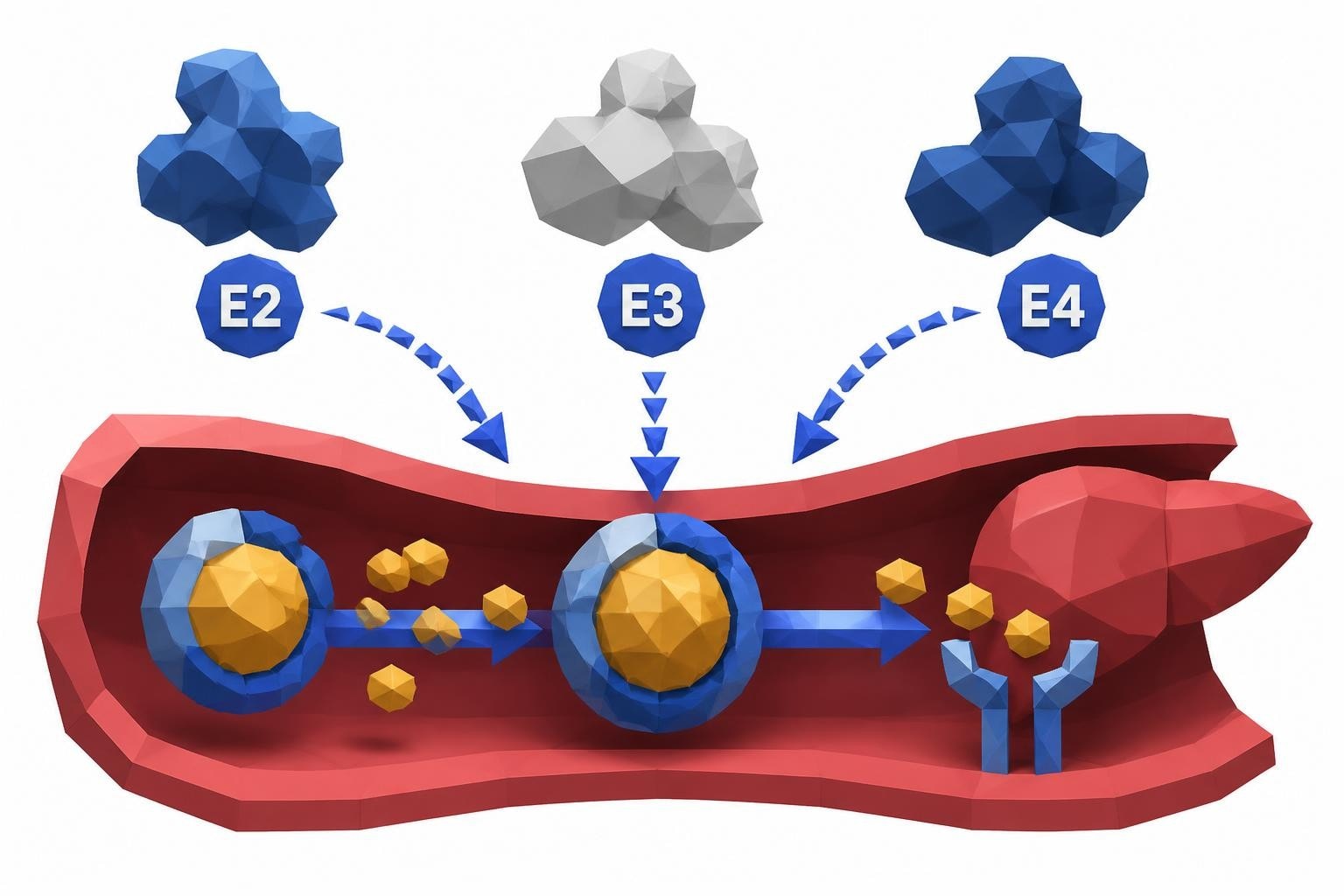
The ApoE genotype test represents another valuable genetic assessment, revealing variants affecting cardiovascular disease risk and Alzheimer's disease susceptibility. Different ApoE variants influence how efficiently the body clears cholesterol-containing particles from circulation.
Managing Inherited Lipoprotein Risks
Discovering elevated lipoprotein genetic health risj factors demands action rather than resignation. While you cannot change your genes, you can substantially modify how they impact long-term health outcomes through targeted interventions.
Lifestyle Modifications
Even genetically determined lipoprotein disorders respond to lifestyle optimization:
- Dietary adjustments emphasizing plant-based foods, fiber, and healthy fats can improve overall lipid profiles
- Regular physical activity enhances HDL function and improves triglyceride clearance
- Weight management reduces inflammation and metabolic stress on lipoprotein processing systems
- Smoking cessation eliminates a major synergistic risk factor that amplifies genetic vulnerabilities
- Stress reduction lowers cortisol-driven metabolic dysfunction affecting lipid metabolism
For individuals with elevated Lp(a), these lifestyle measures primarily address other cardiovascular risk factors since Lp(a) levels themselves resist modification through diet and exercise.
Pharmaceutical Interventions
Modern medications offer powerful tools for managing genetic lipoprotein disorders:
Statins remain first-line therapy for elevated LDL cholesterol, effectively lowering levels by 30-50% regardless of genetic cause. They work by inhibiting cholesterol synthesis, forcing the liver to increase LDL receptor production for enhanced particle clearance.
PCSK9 inhibitors represent breakthrough medications for familial hypercholesterolemia and other severe genetic cholesterol disorders. These injectable biologics can reduce LDL cholesterol by an additional 50-60% beyond statin therapy, preventing cardiovascular events in high-risk individuals.
Ezetimibe blocks cholesterol absorption in the intestines, providing complementary LDL reduction when combined with statins. This oral medication proves particularly useful for individuals unable to tolerate high-dose statin therapy.
| Medication Class | Mechanism | Typical LDL Reduction | Special Considerations |
|---|---|---|---|
| Statins | Inhibit cholesterol synthesis | 30-50% | First-line therapy, proven outcomes |
| PCSK9 Inhibitors | Enhance LDL clearance | 50-60% | Injectable, expensive, very effective |
| Ezetimibe | Block absorption | 15-25% | Oral, well-tolerated, additive effect |
| Bempedoic Acid | Alternative synthesis inhibitor | 15-25% | Oral, statin-intolerant option |
For elevated Lp(a), treatment options remain limited but evolving. High-intensity statin therapy and PCSK9 inhibitors can modestly reduce Lp(a) levels while substantially lowering LDL cholesterol. Emerging therapies specifically targeting Lp(a) show promise in clinical trials, potentially transforming management of this lipoprotein genetic health risj factor within coming years.
Family Screening and Cascade Testing
When an individual receives a diagnosis of a genetic lipoprotein disorder, cascade screening recommendations from the American Heart Association suggest testing family members to identify others at risk. This systematic approach enables early detection before cardiovascular damage accumulates.
Implementing Family Screening
First-degree relatives-parents, siblings, and children-of someone with familial hypercholesterolemia have a 50% probability of carrying the same genetic mutation. Testing these family members identifies affected individuals who may benefit from early intervention.
For elevated Lp(a), approximately 90% of variation is genetically determined with levels showing high correlation between parents and children. The impact of elevated Lp(a) on heart health makes family screening particularly valuable when one member has very high levels.
Accessible testing makes family screening practical. When relatives can obtain testing without navigating insurance pre-authorization and physician referrals, participation rates increase substantially.
Testing in Children and Adolescents
Professional guidelines recommend cholesterol screening between ages 9-11 for all children, with earlier and more comprehensive testing for those with family histories of premature cardiovascular disease or genetic lipid disorders. Identifying familial hypercholesterolemia in childhood allows decades of preventive therapy before atherosclerosis develops.
Children with one affected parent have elevated cholesterol levels from birth. Early diagnosis enables family education about heart-healthy habits and, when necessary, medication to prevent arterial damage during critical developmental years.
Emerging Science and Future Directions
Research continues expanding understanding of lipoprotein genetic health risj factors and potential interventions. Genetic and pathophysiological mechanisms of Lp(a) remain active investigation areas, revealing how this particle causes cardiovascular damage beyond simple cholesterol deposition.
Novel Therapies in Development
Antisense oligonucleotides targeting Lp(a) production have demonstrated 80-90% reductions in clinical trials. These medications work by blocking messenger RNA that directs Lp(a) synthesis in the liver. Phase 3 trials are evaluating whether these dramatic reductions translate into fewer cardiovascular events.
Small interfering RNA (siRNA) therapies offer another approach to silencing Lp(a) production, with similar efficacy to antisense technology but different dosing schedules. Both platforms represent precision medicine approaches specifically addressing genetic risk factors.
CRISPR-based gene editing techniques remain experimental but hold theoretical potential for permanently correcting genetic mutations causing lipoprotein disorders. Ethical and technical challenges must be addressed before such approaches become clinical realities.
Polygenic Risk Scores
Beyond single-gene disorders, researchers are developing polygenic risk scores that integrate hundreds of genetic variants, each contributing small effects to overall lipoprotein metabolism and cardiovascular risk. These comprehensive genetic assessments may eventually enable highly personalized prevention strategies.
Practical Steps for Risk Assessment
Taking action on lipoprotein genetic health risj begins with information gathering and testing:
- Review family health history systematically, noting any relatives with heart attacks, strokes, or high cholesterol, particularly events occurring before age 55 in men or 65 in women
- Request comprehensive lipid testing including Lp(a) measurement, especially if family history suggests genetic risks
- Consider genetic counseling when multiple family members have premature cardiovascular disease or diagnosed genetic disorders
- Establish baseline measurements early in adulthood to guide long-term prevention strategies
- Share results with family members to encourage their proactive screening and management
Modern testing infrastructure makes obtaining comprehensive lipoprotein profiles straightforward. Results typically become available within 1-3 days, enabling rapid progression from testing to interpretation and action planning.
Recommended Test
Lipoprotein(a)
Lipoprotein(a) is a genetically determined cardiovascular risk factor. Elevated Lp(a) increases your risk of heart disease, stroke, and aortic valve disease independent of LDL cholesterol.
Includes 1 biomarkers
$21
Key takeaways
Understanding your lipoprotein genetic health risj profile represents a powerful tool for cardiovascular disease prevention. Genetic factors like elevated Lp(a) and familial hypercholesterolemia dramatically increase heart attack and stroke risks, yet many affected individuals remain undiagnosed until after experiencing cardiovascular events. Comprehensive lipid testing extending beyond basic cholesterol panels reveals these hidden genetic vulnerabilities, enabling targeted interventions decades before symptoms appear. Family screening multiplies the value of genetic testing by identifying at-risk relatives who benefit from early detection. While you cannot change inherited genes, you can substantially modify their health impacts through informed lifestyle choices, appropriate medications, and proactive monitoring. Accessible testing options remove traditional barriers, making advanced cardiovascular risk assessment available to anyone concerned about genetic lipoprotein disorders.
FAQ
What is the difference between regular cholesterol and lipoprotein genetic risks?
Regular cholesterol levels fluctuate based on diet, exercise, medications, and other modifiable factors. Genetic lipoprotein risks like elevated Lp(a) or familial hypercholesterolemia are primarily determined by inherited DNA variations and remain relatively stable regardless of lifestyle modifications. While standard cholesterol responds well to dietary changes and exercise, genetic lipoprotein disorders typically require pharmaceutical interventions for adequate management. Both standard cholesterol and genetic factors contribute to overall cardiovascular risk, but genetic markers often exert stronger effects and require different management approaches.
How often should I test for genetic lipoprotein risks?
Lipoprotein(a) requires testing only once in a lifetime since levels are genetically determined and remain stable throughout adulthood. However, if your initial Lp(a) test occurs during pregnancy or active inflammation, retesting after these conditions resolve ensures accuracy. For other genetic lipoprotein disorders like familial hypercholesterolemia, initial diagnosis involves cholesterol testing, but monitoring frequency depends on treatment status. Treated individuals typically retest every 3-6 months until levels stabilize, then annually for ongoing monitoring. Untreated individuals with known genetic risks should obtain testing annually to guide treatment decisions.
Can diet and exercise lower genetically high Lp(a) levels?
Unfortunately, Lp(a) levels resist modification through diet, exercise, or most conventional cholesterol medications. Lifestyle changes cannot overcome the genetic programming that determines Lp(a) production. However, this does not mean lifestyle modifications are unimportant for individuals with elevated Lp(a). Healthy habits address other cardiovascular risk factors, preventing synergistic damage when multiple risks combine. Optimal diet, regular exercise, smoking avoidance, blood pressure control, and diabetes prevention remain critical for minimizing overall cardiovascular risk despite unchangeable Lp(a) levels. Emerging pharmaceutical therapies specifically targeting Lp(a) show promise for those needing risk reduction beyond lifestyle optimization.
Should my children be tested if I have a genetic lipoprotein disorder?
Yes, children of parents with diagnosed genetic lipoprotein disorders should undergo testing. For familial hypercholesterolemia, screening between ages 9-11 enables early detection and intervention before atherosclerosis develops. Children with affected parents have a 50% chance of inheriting the condition, making screening highly valuable. For elevated Lp(a), testing provides lifelong risk information that guides cardiovascular prevention strategies. Early awareness allows families to emphasize heart-healthy habits from childhood and enables healthcare providers to monitor for early signs of cardiovascular disease. Knowing genetic status eliminates uncertainty and supports informed health decisions throughout life.
What Lp(a) level is considered dangerous?
Cardiovascular risk increases progressively with rising Lp(a) levels rather than following a sharp threshold. Generally, levels below 30 mg/dL are considered desirable with minimal genetic risk. Levels between 30-50 mg/dL represent borderline elevation with moderately increased risk. Levels above 50 mg/dL indicate significant elevation warranting aggressive management of other cardiovascular risk factors. Extremely elevated levels above 100 mg/dL confer very high genetic risk and may prompt consideration of emerging Lp(a)-lowering therapies. However, risk interpretation requires context including other cardiovascular risk factors, family history, and presence of existing heart disease. Healthcare providers integrate Lp(a) results with comprehensive risk assessment to guide personalized prevention strategies.
Are genetic lipoprotein tests covered by insurance?
Insurance coverage for genetic lipoprotein testing varies significantly by plan and clinical indication. Lp(a) testing may be covered when ordered for specific indications like premature cardiovascular disease, recurrent events despite treatment, or strong family history. However, many insurers consider it screening rather than diagnostic testing and deny coverage for asymptomatic individuals. Genetic testing for familial hypercholesterolemia typically receives coverage when clinical presentation suggests inherited disorders. Rather than navigating complex insurance pre-authorization processes, many individuals choose direct-access testing with transparent, affordable pricing that often costs less than insurance copays and deductibles while providing faster results.
Proactive assessment of lipoprotein genetic health risj factors enables targeted cardiovascular disease prevention decades before symptoms emerge. Understanding your inherited risks through comprehensive testing empowers informed decisions about lifestyle optimization and medical interventions. Justlabs makes advanced lipoprotein screening accessible with transparent pricing, no insurance hassles, and results delivered in 1-3 days, helping you take control of your cardiovascular health today.