Understanding your cholesterol levels involves more than knowing your total cholesterol or LDL numbers. Lipoprotein(a), commonly abbreviated as Lp(a), represents a critical yet frequently overlooked cardiovascular risk factor that affects approximately 20% of the global population. Unlike traditional cholesterol markers that respond to diet and lifestyle changes, Lp(a) levels are primarily determined by genetics, making early detection through testing essential for cardiovascular disease prevention. The lpa cholesterol risk you face remains constant throughout your life, unaffected by the healthy habits that typically lower other cholesterol types.
What Makes Lp(a) Different from Regular Cholesterol
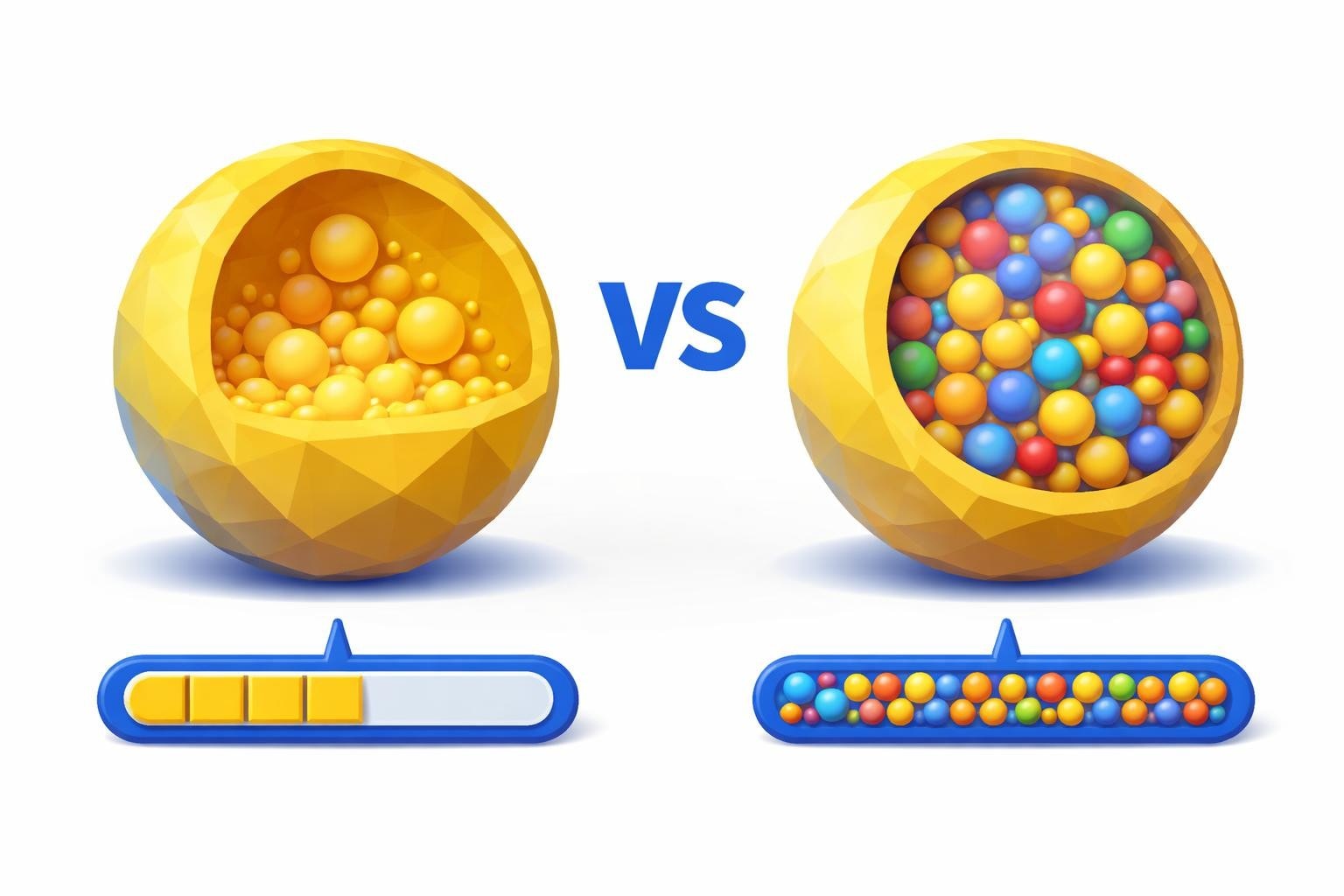
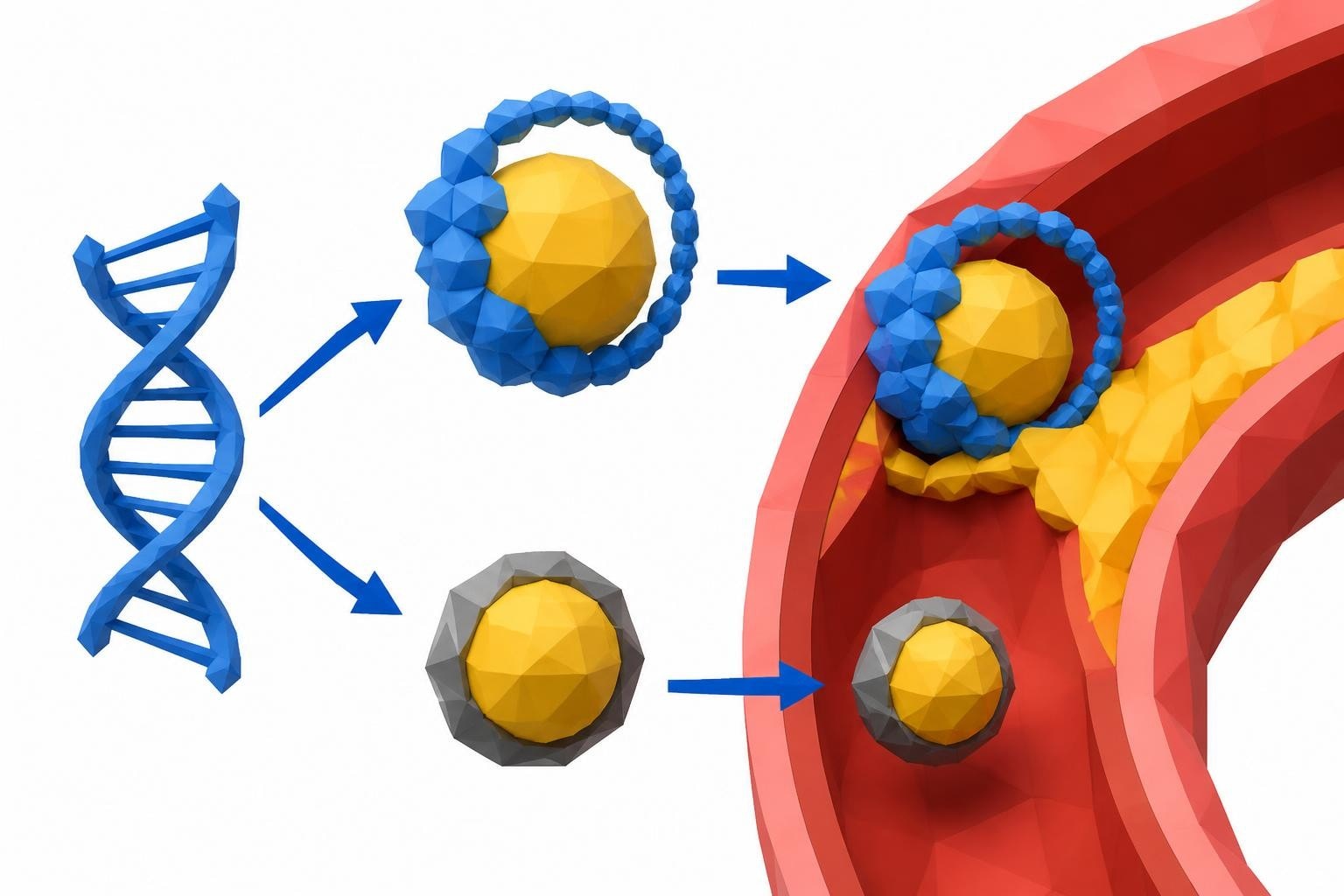
Lp(a) consists of an LDL particle attached to an additional protein called apolipoprotein(a). This unique structure distinguishes it from standard LDL cholesterol in significant ways.
The Genetic Nature of Lp(a)
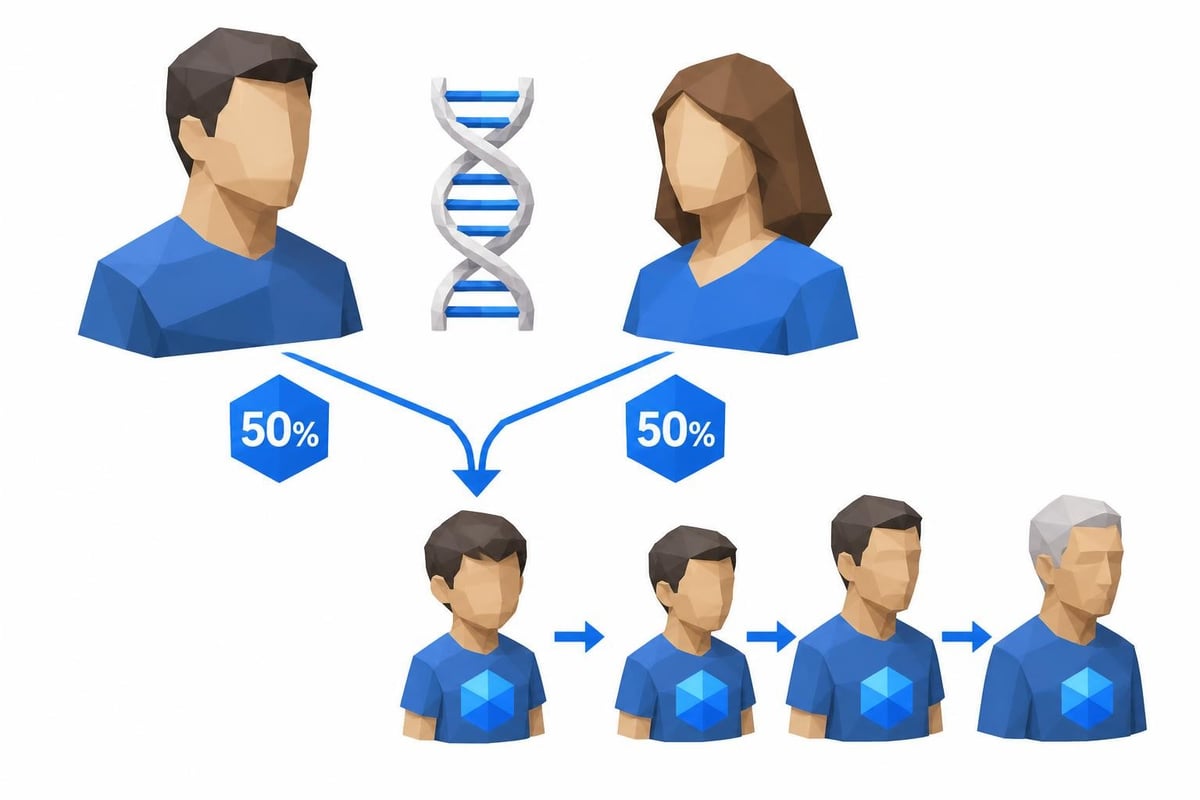
Your Lp(a) level is determined almost entirely by the genes you inherit from your parents. According to the National Heart, Lung, and Blood Institute, approximately 80-90% of Lp(a) variation between individuals comes from genetic factors. This means:
- Diet modifications have minimal impact on Lp(a) levels
- Exercise does not significantly reduce Lp(a)
- Weight loss typically does not change Lp(a) concentrations
- Your levels remain relatively stable throughout adulthood
The genetic determination of Lp(a) makes it fundamentally different from LDL cholesterol, which responds to lifestyle interventions. If one of your parents has elevated Lp(a), you have a 50% chance of inheriting that trait.
How Lp(a) Damages Your Arteries
Lp(a) promotes cardiovascular disease through multiple mechanisms. The particle penetrates artery walls more easily than regular LDL cholesterol, contributing to plaque formation. Beyond this atherosclerotic effect, Lp(a) also promotes inflammation and interferes with the body's natural clot-dissolving processes.
| Lp(a) Risk Mechanism | Impact on Cardiovascular Health |
|---|---|
| Plaque Formation | Accelerates atherosclerosis development |
| Inflammation | Promotes arterial wall damage |
| Thrombosis | Increases blood clot formation risk |
| Oxidation | Enhances oxidative stress in vessel walls |
These combined effects explain why elevated Lp(a) independently increases your risk for heart attacks, strokes, and aortic valve disease even when other cholesterol numbers look normal.
Understanding Your Lpa Cholesterol Risk Levels
Testing for Lp(a) provides crucial information about your cardiovascular risk profile. Unlike LDL cholesterol, which has treatment targets, Lp(a) measurement primarily serves to stratify risk and guide preventive strategies.
What the Numbers Mean
Lp(a) levels are typically measured in milligrams per deciliter (mg/dL) or nanomoles per liter (nmol/L). The American Heart Association considers levels above 50 mg/dL (approximately 125 nmol/L) as elevated and associated with increased cardiovascular risk.
Risk Categories:
- Optimal: Less than 30 mg/dL (75 nmol/L)
- Borderline: 30-50 mg/dL (75-125 nmol/L)
- High: Above 50 mg/dL (125 nmol/L)
- Very High: Above 100 mg/dL (250 nmol/L)
Individuals with very high Lp(a) levels face a cardiovascular risk equivalent to someone with familial hypercholesterolemia, a severe inherited cholesterol disorder. This substantial lpa cholesterol risk often goes undetected because Lp(a) is not included in standard cholesterol panels.
Who Should Get Tested
The growing awareness of Lp(a) has prompted experts to recommend broader testing. You should strongly consider Lp(a) testing if you have:
- A personal history of premature cardiovascular disease (before age 55 in men, 65 in women)
- A family history of early heart attacks or strokes
- Recurrent cardiovascular events despite statin treatment
- A family member with known elevated Lp(a)
- Unexplained high cardiovascular risk based on traditional factors
- Ancestry from populations with higher Lp(a) prevalence
Because Lp(a) remains stable throughout life, you only need to test once. If you're concerned about lab test pricing, direct-to-consumer options make this important screening more accessible than ever.
The Clinical Impact of Elevated Lp(a)
Research over the past decade has solidified Lp(a)'s role as a major cardiovascular risk factor. Understanding the specific conditions linked to elevated Lp(a) helps contextualize why testing matters.
Heart Attack and Stroke Risk
Elevated Lp(a) doubles or triples your risk of heart attack and stroke compared to individuals with normal levels. National Geographic's health coverage emphasizes how this risk factor operates independently of other cholesterol markers, meaning you can have perfect LDL and HDL numbers yet still face significant cardiovascular danger.
The lpa cholesterol risk becomes particularly concerning when combined with other risk factors such as high blood pressure, diabetes, or smoking. This multiplicative effect means that managing other modifiable risk factors becomes even more critical when Lp(a) is elevated.
Aortic Valve Disease
Beyond arterial blockages, high Lp(a) levels contribute to calcific aortic valve stenosis, a condition where the heart's aortic valve becomes narrowed and stiff. This connection was surprising to researchers because it demonstrates that Lp(a) affects multiple parts of the cardiovascular system.
Studies indicate that individuals with Lp(a) levels above 50 mg/dL have approximately twice the risk of developing aortic stenosis requiring valve replacement. This relationship exists across different age groups and ethnic backgrounds.
Peripheral Artery Disease
Lp(a) also increases the risk of peripheral artery disease (PAD), where arteries in the legs become narrowed or blocked. Patients with both elevated Lp(a) and PAD face higher rates of limb complications and cardiovascular events.
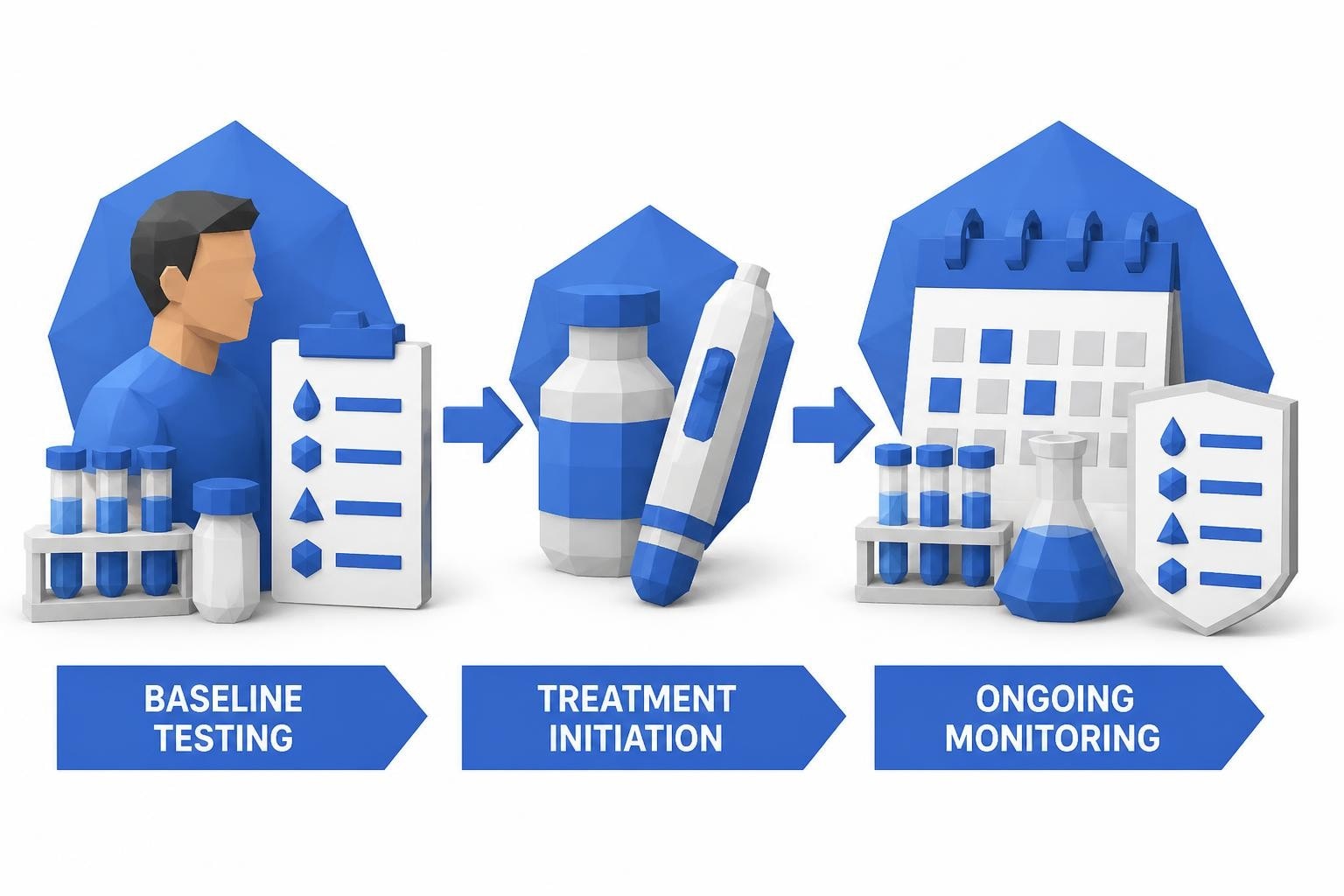
Managing Your Lp(a) Risk
While you cannot change your genetic Lp(a) level through diet or exercise, knowing your status enables targeted risk reduction strategies. The goal shifts from lowering Lp(a) itself to aggressively managing all other cardiovascular risk factors.
Optimizing Other Risk Factors
When you have elevated Lp(a), your physician may recommend more aggressive treatment of modifiable risk factors:
- LDL Cholesterol: Target levels below 70 mg/dL or even 55 mg/dL through statins or other medications
- Blood Pressure: Maintain levels below 130/80 mmHg
- Blood Sugar: Achieve optimal glycemic control if diabetic or prediabetic
- Smoking: Complete cessation, as smoking dramatically amplifies lpa cholesterol risk
- Weight: Maintain a healthy body mass index
- Physical Activity: Regular aerobic and resistance exercise
| Risk Factor | Standard Target | Enhanced Target with High Lp(a) |
|---|---|---|
| LDL Cholesterol | <100 mg/dL | <70 mg/dL or <55 mg/dL |
| Blood Pressure | <140/90 mmHg | <130/80 mmHg |
| A1C (if diabetic) | <7.0% | <6.5% |
| BMI | <25 | <23 |
These enhanced targets compensate for the non-modifiable lpa cholesterol risk by minimizing all other cardiovascular threats.
Medications and Emerging Therapies
Currently available medications have limited effects on Lp(a) levels. High-dose niacin can reduce Lp(a) by 20-30%, but this approach has fallen out of favor due to side effects and lack of proven cardiovascular benefit. PCSK9 inhibitors, powerful LDL-lowering drugs, reduce Lp(a) by approximately 25-30% as a secondary effect.
The most promising development involves antisense oligonucleotide therapies specifically targeting Lp(a) production. These experimental treatments can reduce Lp(a) levels by 80-90% and are currently in late-stage clinical trials. Results expected in 2027 may revolutionize how we manage this risk factor.
Aspirin and Antiplatelet Therapy
Because Lp(a) promotes blood clotting, some physicians recommend low-dose aspirin for patients with significantly elevated levels. This decision requires individual assessment, balancing cardiovascular risk reduction against bleeding risk. Time magazine's coverage discusses how personalized approaches to Lp(a) management are evolving as research progresses.
Why Lp(a) Testing Remains Underutilized
Despite compelling evidence of its importance, Lp(a) testing is not routinely performed in standard cholesterol screening. Several factors contribute to this gap in care.
Cost and Accessibility Barriers
Traditional healthcare systems often require specific physician orders for Lp(a) testing, and insurance coverage varies widely. Many patients face obstacles getting tested even when they specifically request it. However, the landscape is changing as direct access to lab testing removes these barriers, allowing individuals to proactively assess their cardiovascular risk.
The one-time nature of Lp(a) testing makes it cost-effective over a lifetime. Unlike cholesterol panels that require periodic monitoring, a single Lp(a) test provides permanent risk information because levels do not significantly change.
Physician Awareness
Many healthcare providers remain unfamiliar with Lp(a) testing guidelines and interpretation. Medical education has historically focused on LDL and HDL cholesterol, with Lp(a) receiving minimal attention. This knowledge gap means patients often need to advocate for their own testing.
As patient stories shared by the American Heart Association demonstrate, individuals who proactively requested Lp(a) testing have discovered significant risk factors that explained family histories of heart disease.
Treatment Limitations
The historical lack of specific Lp(a)-lowering therapies contributed to clinical reluctance around testing. The reasoning was that identifying a problem without a solution created anxiety without benefit. However, this perspective has shifted as evidence shows that knowing your Lp(a) status guides more aggressive management of other risk factors and can prevent cardiovascular events.
Ethnic and Population Differences in Lp(a) Levels
Lp(a) levels vary significantly across different ancestral populations. Understanding these patterns helps identify individuals who might benefit most from testing.
Population Variations:
- Individuals of African descent have median Lp(a) levels 2-3 times higher than those of European descent
- South Asian populations show intermediate levels with high variability
- East Asian populations generally have lower median levels
- Hispanic populations demonstrate significant variation based on genetic ancestry
These differences are genetically determined and reflect evolutionary history rather than lifestyle factors. The elevated prevalence in some populations means that ancestry should factor into testing decisions.
Importantly, the relationship between Lp(a) levels and cardiovascular risk appears consistent across ethnic groups, even though baseline levels differ. This means someone of African ancestry with Lp(a) of 60 mg/dL faces similar relative risk as someone of European ancestry at the same level.
Family Screening and Cascade Testing
When an individual tests positive for elevated Lp(a), family screening becomes highly valuable. The genetic inheritance pattern means that siblings and children have a 50% probability of also having high levels.
Implementing Family Screening
Cascade testing involves systematically testing blood relatives when a family member has confirmed elevated Lp(a). This approach efficiently identifies at-risk individuals who can then implement preventive strategies decades before cardiovascular symptoms appear.
The process typically follows this sequence:
- Index patient discovers elevated Lp(a) through testing
- First-degree relatives (parents, siblings, children) undergo testing
- Relatives with elevated levels inform their own children/siblings
- Testing continues through family branches
This systematic approach maximizes the preventive value of a single Lp(a) discovery. Given that testing can be done conveniently through services offering labs without insurance, financial barriers need not prevent family-wide screening.
Children and Adolescents
Because Lp(a) levels stabilize in early childhood, testing children with a family history of elevated Lp(a) can provide valuable information. While cardiovascular disease doesn't manifest until adulthood, knowing a child's status allows for:
- Emphasis on healthy lifestyle habits from an early age
- Monitoring of other risk factors as they grow
- Informed medical care as they transition to adult healthcare
- Awareness that guides personal health decisions
Some experts recommend testing children of affected parents after age 10, while others suggest waiting until late adolescence when results can inform adult health planning.
Getting Tested for Lp(a)
Accessing Lp(a) testing has become significantly easier with the growth of direct-to-consumer lab services. Understanding your options helps you take action on this important health marker.
Testing Methods
Lp(a) is measured through a standard blood draw, similar to regular cholesterol testing. No fasting is required, making it convenient to add to other lab work. The test measures either mass concentration (mg/dL) or particle number (nmol/L), with particle number considered more standardized across different assays.
Results are typically available within a few days. Once you have your number, it provides permanent risk stratification since Lp(a) levels remain stable throughout adult life.
Direct Access Testing Options
Rather than waiting for a physician order, you can order lab tests online directly and visit a nearby collection facility at your convenience. This approach offers several advantages:
- Immediate access without appointment delays
- Transparent pricing known upfront
- Results delivered quickly, often within 1-3 days
- Privacy and convenience for proactive health management
For those who have faced obstacles getting Lp(a) testing through traditional healthcare channels, direct access removes these barriers and empowers personal health decisions.
Recommended Test
Lipoprotein(a)
Lipoprotein(a) is a genetically determined cardiovascular risk factor. Elevated Lp(a) increases your risk of heart disease, stroke, and aortic valve disease independent of LDL cholesterol.
Includes 1 biomarkers
$21
Interpreting Your Results
After receiving your Lp(a) results, consultation with a healthcare provider helps contextualize the findings within your overall cardiovascular risk profile. Even if levels are elevated, remember that this is one component of total risk. The information guides prevention strategies rather than representing an immediate crisis.
Understanding whether your results are reported in mg/dL or nmol/L is important for accurate interpretation. A rough conversion: 1 mg/dL equals approximately 2.5 nmol/L, though this varies based on individual Lp(a) particle size.
The Future of Lp(a) Management
The cardiovascular medicine field is experiencing a significant shift in how Lp(a) is viewed and managed. Research advances promise to transform this from an identified risk to a treatable condition.
Investigational Therapies
Multiple pharmaceutical companies are developing targeted Lp(a)-lowering therapies. Antisense oligonucleotides that prevent Lp(a) production show remarkable efficacy in early studies, with reductions exceeding 80%. Clinical trials are evaluating whether lowering Lp(a) translates to reduced cardiovascular events, with results expected within the next few years.
Small interfering RNA (siRNA) therapies represent another promising approach, using a different mechanism to achieve similar Lp(a) reduction. These treatments require infrequent dosing, potentially every 3-6 months, making them practical for long-term management.
Screening Guideline Evolution
Professional medical societies are increasingly recommending broader Lp(a) screening. Some experts advocate for universal testing at least once in adulthood, similar to the approach for other genetic conditions. As testing becomes more accessible and specific therapies emerge, lpa cholesterol risk assessment may become a standard component of preventive cardiovascular care.
The National Lipid Association provides detailed clinical guidance for healthcare providers on when to test and how to manage elevated Lp(a), reflecting the growing clinical emphasis on this biomarker.
Personalized Risk Prediction
Advanced cardiovascular risk calculators now incorporate Lp(a) levels alongside traditional factors like age, blood pressure, and cholesterol. This personalized approach provides more accurate 10-year and lifetime cardiovascular risk estimates, allowing for tailored prevention strategies.
Genetic risk scores that include Lp(a) variants along with hundreds of other genetic markers may further refine risk prediction, though current evidence supports direct Lp(a) measurement as the most clinically useful approach.
Proactive cardiovascular health management starts with knowing your complete risk profile, and Lp(a) represents a critical piece that standard screening often misses. Whether you have a family history of heart disease, experienced an early cardiovascular event, or simply want comprehensive health information, testing for Lp(a) provides valuable insights that guide prevention strategies. Justlabs makes this important screening accessible and affordable, with transparent pricing and convenient online ordering that delivers results in 1-3 days, empowering you to take control of your cardiovascular health without navigating insurance barriers or waiting for doctor appointments.