Experiencing persistent joint pain, especially when accompanied by morning stiffness and swelling, can be more than just a sign of aging or overuse. When joints in your hands, wrists, or feet become tender and inflamed, rheumatoid factor joint pain may be the underlying cause. This autoimmune response occurs when your immune system mistakenly produces antibodies called rheumatoid factor that attack healthy joint tissue, leading to chronic inflammation and progressive damage. Understanding the connection between rheumatoid factor and joint symptoms is crucial for early diagnosis and effective treatment of rheumatoid arthritis.
What Is Rheumatoid Factor and How Does It Cause Joint Pain
Rheumatoid factor (RF) is an autoantibody, meaning it's an antibody that targets your own body's tissues rather than foreign invaders like bacteria or viruses. Specifically, RF attacks immunoglobulin G (IgG), a normal antibody found in your blood.
When rheumatoid factor accumulates in joint spaces, it triggers a cascade of inflammatory responses. The presence of these autoantibodies activates immune cells that release inflammatory chemicals called cytokines. These chemicals cause the synovium-the thin membrane lining your joints-to become inflamed and thickened.
Over time, this chronic inflammation leads to several damaging processes:
- Cartilage breakdown: The protective cushioning between bones deteriorates
- Bone erosion: Joint surfaces become damaged and irregular
- Synovial proliferation: The joint lining grows abnormally thick
- Fluid accumulation: Excess fluid builds up, causing swelling and stiffness
The symptoms of rheumatoid arthritis typically develop gradually, though some people experience rapid onset. The resulting rheumatoid factor joint pain differs from ordinary arthritis pain because it stems from active autoimmune attack rather than simple wear and tear.
The Connection Between RF Levels and Pain Severity
Not everyone with elevated rheumatoid factor experiences the same degree of joint pain. Research indicates that higher RF levels often correlate with more aggressive disease and greater joint damage, though this relationship isn't absolute.
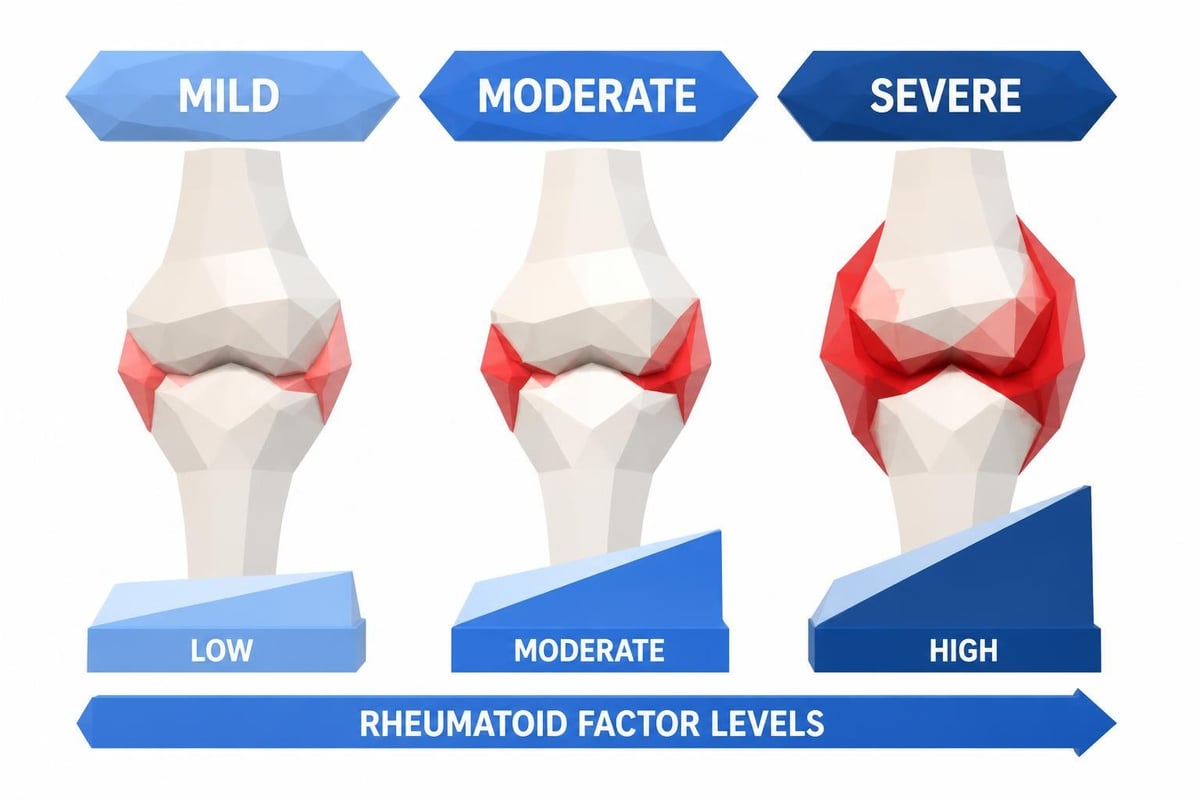
Patients with very high RF levels tend to experience:
- More pronounced morning stiffness lasting over an hour
- Greater number of affected joints throughout the body
- Increased risk of extra-articular manifestations
- Higher likelihood of requiring aggressive treatment
- Faster progression of structural joint damage
However, approximately 20-30% of people with rheumatoid arthritis test negative for rheumatoid factor yet still develop significant joint pain and damage. This condition is called seronegative rheumatoid arthritis, demonstrating that RF testing provides valuable but not definitive diagnostic information.
Recognizing the Distinct Characteristics of Rheumatoid Factor Joint Pain
Rheumatoid factor joint pain presents with specific patterns that help distinguish it from other types of arthritis. Understanding these characteristics enables earlier recognition and diagnosis.
Symmetrical Joint Involvement
Unlike osteoarthritis, which often affects one side of the body more than the other, rheumatoid factor joint pain typically manifests symmetrically. If your right wrist becomes inflamed, your left wrist will likely develop similar symptoms within a similar timeframe.
This symmetrical pattern reflects the systemic nature of the autoimmune response. The Arthritis Foundation provides comprehensive information about how rheumatoid arthritis affects the entire body rather than isolated joints.
| Joint Location | Frequency of Involvement | Typical Symptoms |
|---|---|---|
| Hands (MCP, PIP joints) | 80-90% of cases | Swelling, warmth, reduced grip strength |
| Wrists | 75-85% of cases | Limited range of motion, tenderness |
| Feet (MTP joints) | 70-80% of cases | Pain when walking, swelling |
| Knees | 60-70% of cases | Effusion, difficulty bending |
| Shoulders | 50-60% of cases | Reduced mobility, nighttime pain |
Morning Stiffness and the Gel Phenomenon
One hallmark of rheumatoid factor joint pain is prolonged morning stiffness, often lasting 30 minutes to several hours. This differs significantly from osteoarthritis, where stiffness typically resolves within 15-30 minutes of activity.
The "gel phenomenon" describes how joints affected by rheumatoid factor become particularly stiff after periods of inactivity. Getting out of bed in the morning or rising from a chair after sitting becomes progressively difficult as the day begins.
When to Consider Rheumatoid Factor Testing
Understanding when to pursue lab testing for rheumatoid factor can accelerate diagnosis and treatment initiation. Early detection significantly improves long-term outcomes for people with rheumatoid arthritis.
Warning Signs That Warrant Testing
Several symptoms and patterns should prompt consideration of rheumatoid factor testing:
- Persistent joint pain affecting small joints of the hands or feet for more than six weeks
- Morning stiffness lasting longer than one hour
- Symmetrical joint involvement with similar symptoms on both sides of the body
- Unexplained fatigue that doesn't improve with rest
- Low-grade fever without obvious infection
- Family history of rheumatoid arthritis or other autoimmune conditions
For those experiencing these symptoms, ordering lab tests without a doctor's visit can provide quick answers and help determine whether medical consultation is necessary. This approach offers convenience and transparency while reducing delays in potential diagnosis.
Understanding the Testing Process
Rheumatoid factor testing requires a simple blood draw. The test measures the concentration of RF antibodies in your blood, typically reported in international units per milliliter (IU/mL).
Standard interpretation guidelines include:
- Less than 15 IU/mL: Generally considered negative
- 15-20 IU/mL: Borderline or weakly positive
- 20-60 IU/mL: Moderately positive
- Greater than 60 IU/mL: Strongly positive
Results typically become available within 1-3 days through services like Justlabs, which provides fast turnaround times and transparent pricing. However, interpreting rheumatoid factor results requires context beyond just the numerical value.
Interpreting Rheumatoid Factor Results in Context
A positive rheumatoid factor test doesn't automatically mean you have rheumatoid arthritis, nor does a negative result rule it out completely. Understanding how to interpret results requires considering multiple factors.
False Positives and Alternative Explanations
Elevated rheumatoid factor levels can occur in various conditions besides rheumatoid arthritis:
- Other autoimmune diseases: Lupus, Sjögren's syndrome, mixed connective tissue disease
- Chronic infections: Hepatitis C, tuberculosis, endocarditis
- Chronic lung diseases: Pulmonary fibrosis, sarcoidosis
- Liver conditions: Cirrhosis, chronic hepatitis
- Aging: Up to 15% of healthy people over 65 test positive for RF
Additionally, approximately 5% of healthy young adults have detectable rheumatoid factor without any disease. This highlights why rheumatoid factor testing should be combined with clinical evaluation and other diagnostic markers.
Complementary Tests for Comprehensive Assessment
Healthcare providers typically order additional tests alongside rheumatoid factor to build a complete diagnostic picture:
| Test | Purpose | Clinical Significance |
|---|---|---|
| Anti-CCP antibodies | More specific for RA than RF | High specificity (95-98%) for rheumatoid arthritis |
| C-reactive protein (CRP) | Measures inflammation level | Elevated in active disease |
| Erythrocyte sedimentation rate (ESR) | Another inflammation marker | Correlates with disease activity |
| Complete blood count | Detects anemia, infection | Common in RA due to chronic inflammation |
The Harvard Health Publishing resource explains how physicians combine these various markers to distinguish rheumatoid factor joint pain from other causes of joint inflammation.
Managing Rheumatoid Factor Joint Pain Through Treatment
Once diagnosed with rheumatoid arthritis causing rheumatoid factor joint pain, several treatment approaches can significantly reduce symptoms and prevent progressive joint damage.
Disease-Modifying Antirheumatic Drugs (DMARDs)
These medications represent the cornerstone of rheumatoid arthritis treatment because they address the underlying autoimmune process rather than just symptoms.
Conventional DMARDs include:
- Methotrexate (most commonly prescribed first-line therapy)
- Hydroxychloroquine (useful for mild disease)
- Sulfasalazine (often combined with other DMARDs)
- Leflunomide (alternative when methotrexate isn't tolerated)
Biologic DMARDs target specific components of the immune system:
- TNF inhibitors (etanercept, adalimumab, infliximab)
- B-cell depletion therapy (rituximab)
- IL-6 inhibitors (tocilizumab, sarilumab)
- T-cell costimulation blockers (abatacept)
These medications can reduce rheumatoid factor levels over time while decreasing inflammation and preventing joint destruction. Medical News Today provides detailed information about treatment options and how they affect disease progression.
Symptomatic Relief Strategies
While DMARDs work to modify the disease course, several approaches provide more immediate relief from rheumatoid factor joint pain:
- Nonsteroidal anti-inflammatory drugs (NSAIDs): Reduce pain and inflammation
- Corticosteroids: Provide rapid relief during flares
- Physical therapy: Maintains joint function and range of motion
- Occupational therapy: Teaches joint protection techniques
- Heat and cold therapy: Reduces stiffness and pain
- Assistive devices: Reduces stress on affected joints
Monitoring Disease Progression and Treatment Response
Regular monitoring through lab testing helps track how well treatments control rheumatoid factor joint pain and prevent disease progression.
Key Metrics to Track Over Time
Effective disease management requires periodic reassessment of multiple markers:
- Rheumatoid factor levels: May decrease with effective treatment
- Inflammatory markers: CRP and ESR should normalize
- Joint examination: Number of tender and swollen joints
- Patient-reported outcomes: Pain scales, function assessments
- Imaging studies: X-rays or ultrasound to detect structural changes
Most rheumatologists recommend testing inflammatory markers every 3-6 months during treatment. For those managing costs independently, comparing lab test pricing across different providers can make regular monitoring more affordable without sacrificing quality.
Adjusting Treatment Based on Results
Treatment modifications depend on how effectively current therapy controls disease activity:
| Scenario | RF Trend | CRP/ESR | Treatment Adjustment |
|---|---|---|---|
| Excellent response | Decreasing | Normal | Continue current therapy |
| Partial response | Stable or slightly decreased | Mildly elevated | Add or switch DMARDs |
| Poor response | Unchanged or increasing | Significantly elevated | Switch to biologic therapy |
| Remission | Low or negative | Normal | Consider dose reduction |
Achieving and maintaining remission-the state where rheumatoid factor joint pain and inflammation are minimal or absent-represents the primary treatment goal. Studies show that early aggressive treatment leads to better long-term outcomes and reduced joint damage.
The Role of Lifestyle Modifications in Managing Joint Pain
Beyond pharmaceutical interventions, several lifestyle approaches can help reduce rheumatoid factor joint pain and improve overall quality of life.
Anti-Inflammatory Dietary Approaches
While diet alone cannot cure rheumatoid arthritis, certain nutritional strategies may help reduce inflammation:
- Mediterranean diet: Rich in omega-3 fatty acids, fruits, vegetables, and whole grains
- Omega-3 supplementation: May reduce joint tenderness and stiffness
- Limited processed foods: Reduces inflammatory triggers
- Adequate vitamin D: Important for immune function and bone health
Some patients report improvement when eliminating specific trigger foods, though individual responses vary considerably.
Exercise and Physical Activity Considerations
Movement might seem counterintuitive when experiencing rheumatoid factor joint pain, but appropriate exercise provides significant benefits:
- Low-impact aerobic activity: Swimming, cycling, walking
- Range-of-motion exercises: Maintains joint flexibility
- Strengthening exercises: Supports and protects joints
- Balance training: Reduces fall risk
Starting slowly and working with physical therapists familiar with rheumatoid arthritis ensures exercises help rather than harm affected joints.
Understanding Seronegative Rheumatoid Arthritis
Approximately 20-30% of people with rheumatoid arthritis test negative for rheumatoid factor, creating diagnostic challenges. These individuals experience similar rheumatoid factor joint pain patterns despite absent or very low RF levels.
Diagnostic Criteria for Seronegative RA
When rheumatoid factor tests return negative, physicians rely on other criteria:
- Anti-CCP antibodies: Often positive even when RF is negative
- Clinical presentation: Symmetrical polyarthritis with morning stiffness
- Imaging findings: X-ray or ultrasound evidence of joint damage
- Response to treatment: Improvement with DMARDs suggests RA
The 2010 ACR/EULAR classification criteria allow diagnosis based on multiple factors beyond just laboratory values. This comprehensive approach ensures people with seronegative disease receive appropriate treatment.
Prognosis Differences
Research suggests seronegative rheumatoid arthritis may follow a slightly different course than seropositive disease:
- Generally milder disease activity initially
- Slower radiographic progression in some cases
- Potentially better response to certain treatments
- Lower risk of extra-articular manifestations
However, seronegative patients still require prompt treatment to prevent joint damage and maintain function.
The Importance of Early Detection and Intervention
Timing significantly impacts long-term outcomes for people experiencing rheumatoid factor joint pain. The "window of opportunity" refers to the early disease period when aggressive treatment produces the best results.
Studies demonstrate that starting DMARDs within three months of symptom onset leads to:
- Higher rates of remission achievement
- Reduced radiographic progression
- Better functional outcomes
- Lower cumulative joint damage
- Decreased need for joint replacement surgery
This evidence underscores why prompt testing matters when symptoms suggest possible rheumatoid arthritis. Services that provide labs without insurance requirements remove barriers that might otherwise delay diagnosis, enabling faster access to potentially life-changing treatment.
Building Your Healthcare Team
Managing rheumatoid factor joint pain effectively requires coordination among multiple specialists:
- Rheumatologist: Provides specialized care and treatment oversight
- Primary care physician: Coordinates overall health management
- Physical therapist: Develops exercise programs and mobility strategies
- Occupational therapist: Teaches joint protection and adaptive techniques
- Pain management specialist: Addresses persistent pain when standard treatments need supplementation
Regular communication among team members ensures comprehensive care addressing all aspects of the condition.
Understanding rheumatoid factor joint pain empowers you to recognize symptoms early and seek appropriate testing before significant joint damage occurs. Regular monitoring through accessible lab testing helps track disease activity and treatment response, ensuring optimal management over time. If you're experiencing persistent joint symptoms and want answers quickly without insurance hassles or doctor visit delays, Justlabs provides transparent, affordable rheumatoid factor testing with results available in 1-3 days, giving you the information needed to take the next step in protecting your joint health.