Vitamin B12 deficiency remains one of the most commonly misdiagnosed nutritional deficiencies, affecting millions of Americans yet often going undetected through standard blood tests. While conventional B12 serum testing can suggest deficiency, elevated methylmalonic acid levels provide a more definitive marker for identifying true cellular B12 insufficiency. Understanding the connection between methylmalonic acid and b12 deficiency helps both healthcare providers and patients make more informed decisions about testing, diagnosis, and treatment options.
Understanding Methylmalonic Acid as a Biomarker
Methylmalonic acid (MMA) serves as a critical functional marker for vitamin B12 status at the cellular level. Unlike serum B12 tests that measure circulating vitamin levels in the bloodstream, MMA testing reveals whether B12 is actually functioning properly within your cells.
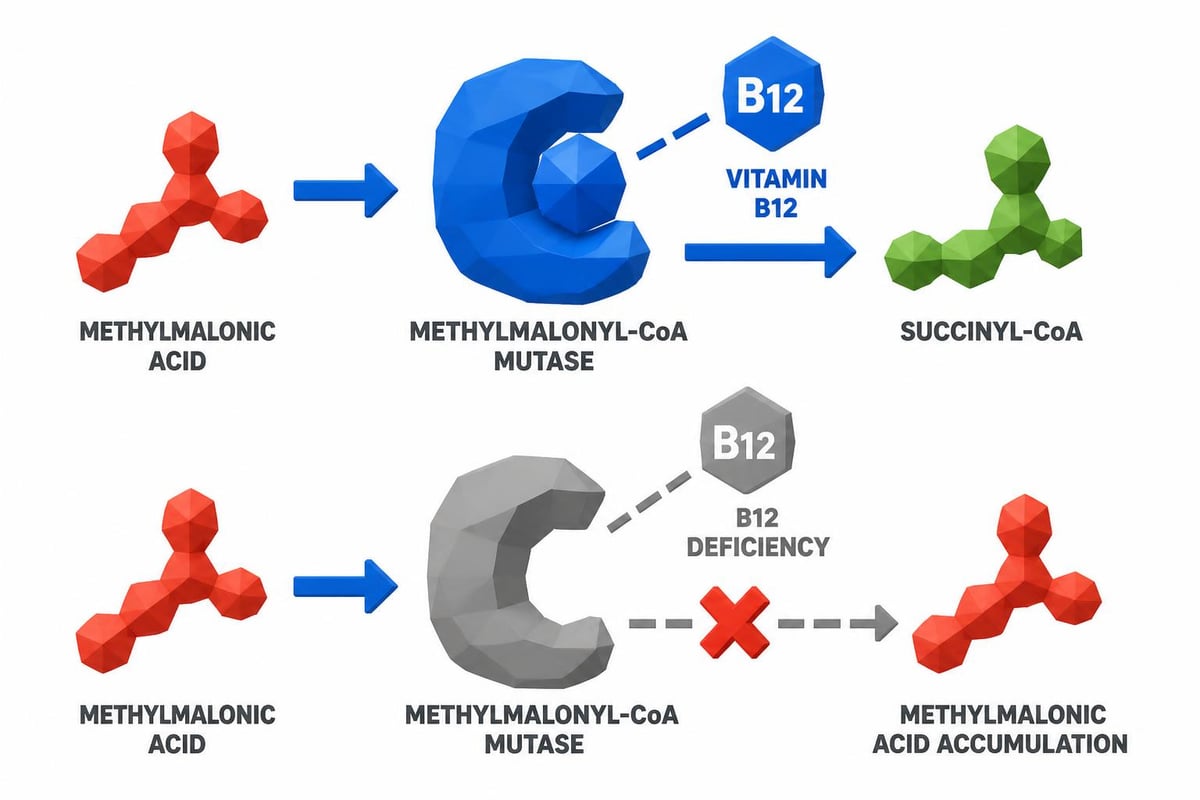
When B12 levels are adequate, the enzyme methylmalonyl-CoA mutase converts methylmalonic acid into succinyl-CoA, a compound essential for energy production and metabolism. However, this enzyme requires vitamin B12 as a cofactor to complete this conversion. When B12 becomes deficient, this enzymatic process cannot proceed efficiently, causing MMA to accumulate in the blood and urine.
How MMA Testing Differs from Standard B12 Tests
Standard serum B12 tests measure total vitamin B12 circulating in your bloodstream, but these tests have significant limitations. According to research on methylmalonic acid testing, serum B12 can appear normal even when cellular deficiency exists.
Key differences include:
- Functional vs. circulating measurement: MMA reveals cellular activity while serum B12 shows blood levels
- Sensitivity: MMA detects earlier stages of deficiency
- Specificity: MMA elevates primarily with B12 deficiency (and kidney disease)
- Clinical accuracy: MMA helps identify subclinical deficiencies
The relationship between methylmalonic acid and b12 deficiency becomes particularly important for patients experiencing neurological symptoms despite normal-appearing B12 levels. MMA testing can reveal functional deficiency when serum tests fail to identify the problem.
Normal Ranges and Interpretation Guidelines
Understanding what constitutes normal versus elevated methylmalonic acid levels helps determine whether B12 deficiency exists and requires treatment. Reference ranges vary slightly between laboratories, but established guidelines provide clear interpretation frameworks.
Standard Reference Ranges
| MMA Level (nmol/L) | Interpretation | Clinical Significance |
|---|---|---|
| 0-270 | Normal | Adequate B12 function |
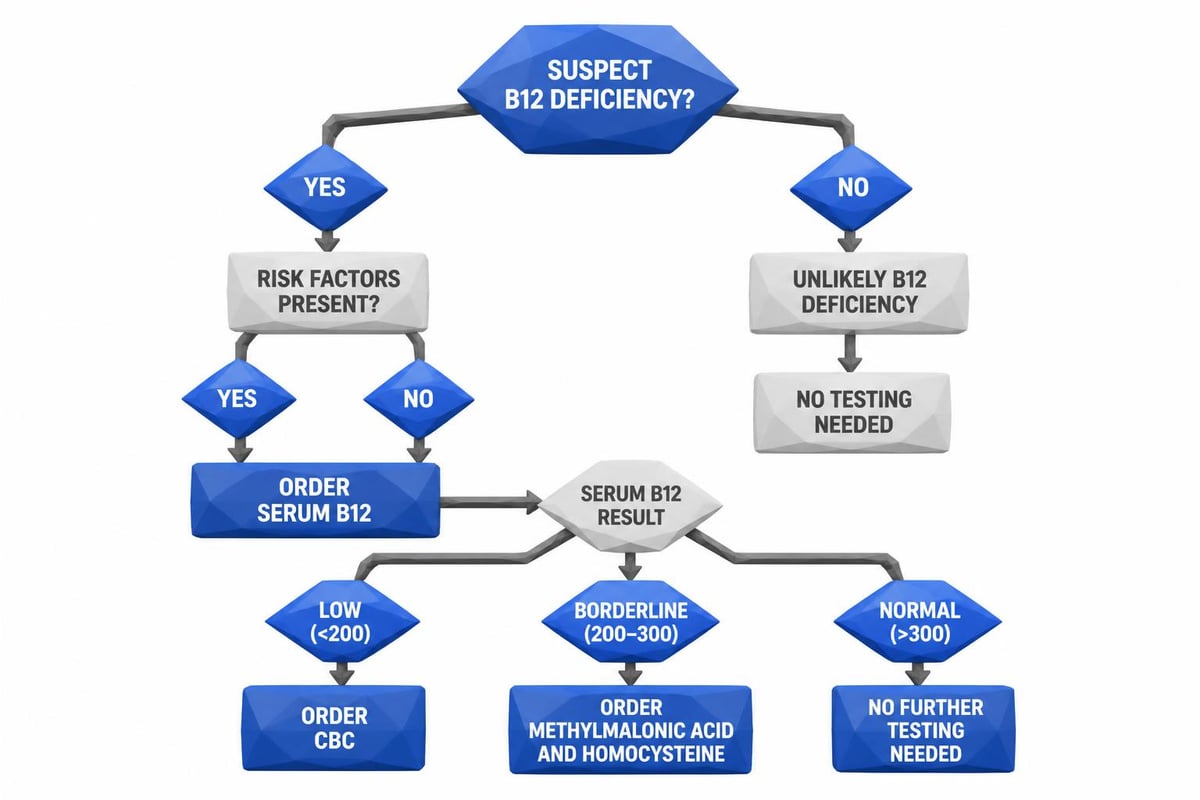
| 271-375 | Borderline | Consider B12 supplementation |
| 376-750 | Moderate elevation | Likely B12 deficiency |
| >750 | Significant elevation | B12 deficiency or kidney disease |
Normal MMA levels typically fall between 70-270 nanomoles per liter (nmol/L) in adults. Values above 270 nmol/L suggest possible B12 deficiency, while levels exceeding 400 nmol/L indicate probable deficiency requiring medical attention.
However, several factors can influence MMA levels beyond B12 status. Kidney disease significantly elevates MMA because impaired renal function prevents proper excretion. Dehydration, certain medications, and rare genetic disorders affecting methylmalonic acid metabolism can also cause elevations unrelated to B12 deficiency.
Clinical Interpretation Considerations
The methylmalonic acid test procedure requires careful interpretation alongside other markers. Physicians typically evaluate MMA results together with:
- Serum B12 levels
- Complete blood count results
- Homocysteine levels
- Renal function tests
- Clinical symptoms and patient history
When both MMA and homocysteine are elevated alongside low or low-normal B12, the diagnosis of B12 deficiency becomes highly reliable. This combination provides stronger diagnostic certainty than any single marker alone.
Causes and Risk Factors for Elevated MMA
Multiple pathways lead to vitamin B12 deficiency and subsequently elevated methylmalonic acid levels. Understanding these causes helps identify who should consider testing and why the connection between methylmalonic acid and b12 deficiency matters for specific populations.
Primary Causes of B12 Deficiency
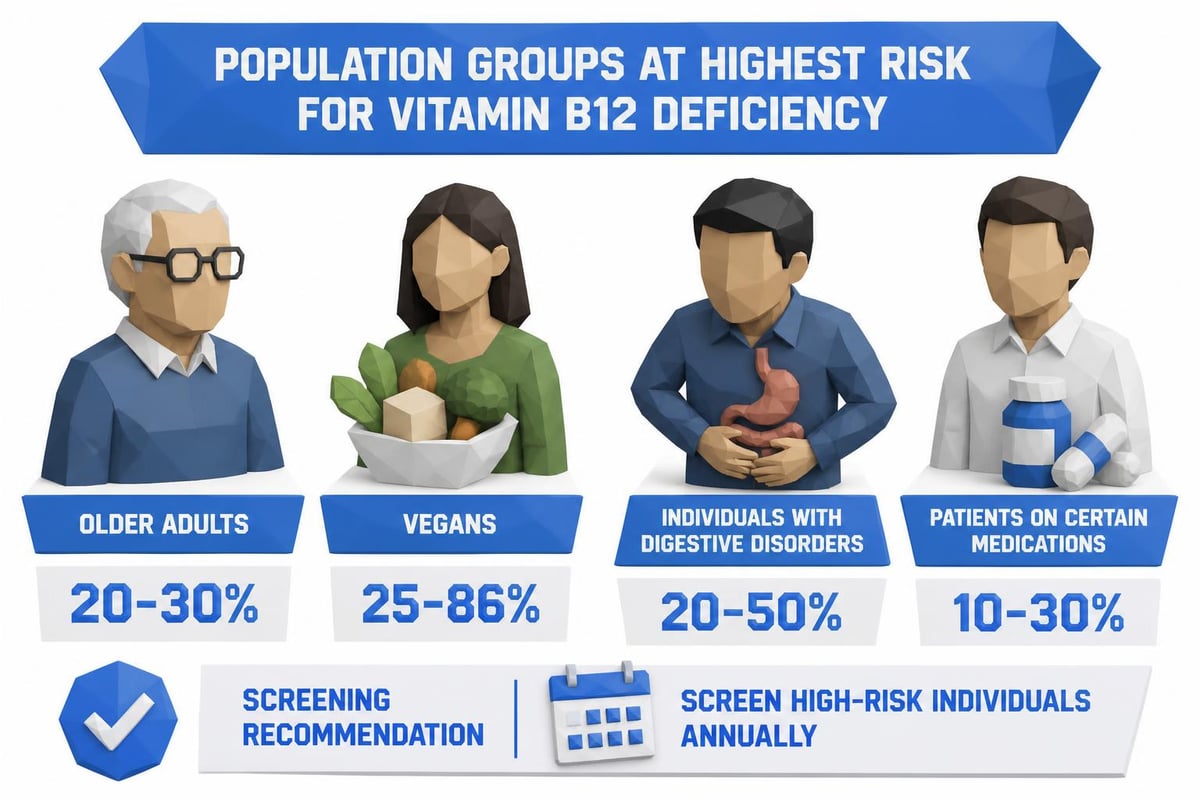
Dietary insufficiency represents the most straightforward cause, particularly affecting strict vegetarians and vegans. Since B12 exists naturally only in animal products, plant-based diets require supplementation or fortified foods to maintain adequate levels.
Malabsorption disorders prevent proper B12 uptake even when dietary intake appears sufficient. Conditions include:
- Pernicious anemia (autoimmune destruction of intrinsic factor)
- Celiac disease and inflammatory bowel disease
- Atrophic gastritis reducing stomach acid production
- Surgical removal of stomach or ileum sections
- Pancreatic insufficiency
Medication interference can block B12 absorption through various mechanisms. Metformin, commonly prescribed for diabetes, reduces B12 absorption in approximately 30% of long-term users. Proton pump inhibitors and H2 blockers decrease stomach acid needed to cleave B12 from food proteins. Some antibiotics and seizure medications also interfere with B12 metabolism.
Age-Related Deficiency
Adults over 50 face increased risk for B12 deficiency due to declining stomach acid production. The National Institutes of Health data on B12 levels indicates that 10-30% of older adults cannot absorb B12 properly from food sources. This population benefits particularly from MMA testing since early deficiency detection prevents irreversible neurological damage.
Clinical Symptoms Warranting MMA Testing
Recognizing symptoms that warrant methylmalonic acid testing enables earlier intervention before permanent damage occurs. B12 deficiency manifests through multiple body systems, creating diverse symptom patterns that vary considerably between individuals.
Neurological and Cognitive Symptoms
The nervous system requires adequate B12 for myelin sheath maintenance and neurotransmitter production. Deficiency symptoms include:
- Numbness and tingling in hands and feet
- Balance problems and difficulty walking
- Memory loss and cognitive decline
- Depression and mood changes
- Confusion and difficulty concentrating
These neurological symptoms can become permanent if deficiency continues untreated. Research has shown connections between B12 deficiency and chronic pain conditions, highlighting the broader neurological implications of inadequate B12 status.
Hematological and Physical Manifestations
B12 deficiency affects blood cell production and overall energy levels. Common physical symptoms include:
- Persistent fatigue and weakness
- Pale or jaundiced skin
- Shortness of breath
- Rapid heartbeat
- Glossitis (inflamed tongue)
- Mouth ulcers
A complete blood count with automated differential often reveals macrocytic anemia, where red blood cells appear larger than normal. However, B12 deficiency can exist without anemia, making MMA testing valuable even when blood counts appear normal.
The Testing Process and Sample Collection
Understanding how methylmalonic acid testing works helps patients prepare appropriately and ensures accurate results. The process differs somewhat from standard blood tests and requires specific considerations.
Preparation Requirements
Most MMA tests require fasting for 8-12 hours before sample collection. This fasting period prevents dietary factors from temporarily influencing results. Water consumption remains acceptable and encouraged during the fasting period.
Certain medications and supplements may need temporary discontinuation before testing. B12 supplements should be stopped at least 48 hours before testing when possible, though this requirement varies based on clinical circumstances and physician recommendations.
Sample Collection Methods
MMA can be measured through either blood or urine samples, though blood testing provides more standardized and reliable results. Blood collection follows standard venipuncture procedures, requiring only a single tube of blood.
The laboratory analysis uses specialized equipment to measure MMA concentration precisely. Results typically become available within 2-5 business days, though timing varies by laboratory. Services like Justlabs provide results within 1-3 days, offering faster turnaround than traditional laboratory channels.
Combined Testing Strategies for Comprehensive Assessment
The relationship between methylmalonic acid and b12 deficiency becomes clearest when MMA testing combines with complementary markers. This comprehensive approach reduces diagnostic uncertainty and guides more effective treatment decisions.
Optimal Testing Panels
| Test Component | Purpose | Interpretation Value |
|---|---|---|
| Serum B12 | Initial screening | Rules out obvious deficiency |
| Methylmalonic Acid | Functional status | Confirms cellular deficiency |
| Homocysteine | Additional marker | Supports diagnosis |
| Complete Blood Count | Anemia detection | Identifies macrocytic changes |
| Creatinine | Kidney function | Rules out renal MMA elevation |
Homocysteine serves as another functional marker for B12 status, though it also elevates with folate deficiency. According to the Pernicious Anaemia Society's analysis, combining MMA and homocysteine testing provides superior diagnostic accuracy compared to either marker alone.
When to Use Comprehensive vs. Targeted Testing
Targeted MMA testing makes sense when B12 deficiency seems likely but serum B12 appears borderline or inconsistent with symptoms. Comprehensive panels work better for:
- Initial diagnostic workup with unclear symptoms
- Monitoring treatment effectiveness
- Evaluating patients with multiple risk factors
- Assessing neurological symptoms of unknown origin
The detailed information about MMA blood testing explains how physicians select appropriate test combinations based on clinical presentation and patient history.
Treatment Monitoring and Follow-Up Testing
After B12 supplementation begins, monitoring methylmalonic acid levels helps verify treatment effectiveness and guide dosage adjustments. MMA responds more slowly than serum B12 to supplementation, but provides more meaningful information about cellular improvement.
Expected Timeline for MMA Reduction
Following B12 treatment initiation, MMA levels typically decrease over several weeks to months:
- Week 1-2: Minimal change in MMA despite rising serum B12
- Week 4-6: MMA begins declining if treatment is adequate
- Month 3-4: MMA approaches normal range with successful treatment
- Month 6+: MMA stabilizes at baseline level
Persistently elevated MMA despite adequate B12 replacement suggests either inadequate dosing, ongoing malabsorption, or rare genetic conditions affecting MMA metabolism. Additional investigation becomes necessary when MMA fails to normalize appropriately.
Adjusting Treatment Based on MMA Results
Treatment protocols vary based on deficiency severity and underlying cause. Mild deficiency may respond to oral supplementation, while severe cases require intramuscular B12 injections.
Monitoring should include repeat MMA testing at:
- 8-12 weeks after starting treatment
- 6 months for continued assessment
- Annually for maintenance verification
- When symptoms recur or new concerns arise
Understanding how to interpret laboratory results helps patients track their progress and communicate effectively with healthcare providers about treatment adjustments.
Accessing MMA Testing Without Traditional Barriers
Traditional healthcare pathways for methylmalonic acid testing often involve multiple physician visits, insurance authorization delays, and extended wait times for appointments and results. Alternative testing approaches provide faster, more convenient access while maintaining diagnostic accuracy.
Direct-Access Laboratory Testing
Self-pay laboratory services enable patients to order lab tests without a doctor's visit, streamlining the testing process significantly. This approach offers several advantages:
- Immediate test ordering without appointment delays
- Transparent, upfront pricing without insurance complications
- Faster result turnaround (typically 1-3 days)
- Digital result delivery for convenient access
- No referral requirements or authorization processes
For patients experiencing symptoms consistent with B12 deficiency or those in high-risk categories, direct laboratory access removes unnecessary barriers to diagnostic testing. This proves particularly valuable when physicians dismiss concerns or when insurance coverage creates prohibitive costs.
Cost Considerations and Transparency
Traditional MMA testing through insurance often involves unpredictable out-of-pocket costs, surprise billing, and complex explanation-of-benefits statements. The transparent lab test pricing model offered by self-pay services provides clear cost expectations upfront.
Price advantages of direct-access testing include:
- No insurance markups: Eliminates the overhead costs insurance companies add
- Bundled pricing: Combined test panels cost less than individual orders
- No surprise bills: Final cost matches quoted price
- Comparison shopping: Ability to evaluate options across providers
Many self-pay testing services accept FSA and HSA payments, allowing patients to use tax-advantaged healthcare dollars for diagnostic testing without involving insurance companies.
Special Populations and Testing Considerations
Certain groups require particular attention regarding the relationship between methylmalonic acid and b12 deficiency due to unique risk factors or testing interpretation challenges.
Pregnancy and Maternal Health
Pregnant women need adequate B12 for fetal neurological development. Deficiency during pregnancy increases risks for neural tube defects and developmental delays. However, pregnancy itself can lower B12 levels temporarily, complicating interpretation.
MMA testing provides more reliable assessment during pregnancy since it reflects functional status rather than just circulating levels affected by plasma volume expansion. Pregnant women following plant-based diets should consider MMA testing regardless of symptoms.
Older Adults and Cognitive Health
The connection between B12 deficiency and cognitive decline makes MMA testing particularly important for older adults experiencing memory problems or dementia symptoms. Studies show that 10-15% of cognitive impairment cases in older adults involve treatable B12 deficiency.
Regular screening after age 60 helps detect deficiency before neurological damage becomes irreversible. MMA testing proves especially valuable because older adults often have borderline B12 levels that don't clearly indicate deficiency without functional markers.
Athletes and Performance Optimization
Athletes require optimal B12 status for energy production, red blood cell formation, and nervous system function. Even marginal deficiency can impair performance, recovery, and training adaptations.
Research on biochemical relationships demonstrates that MMA elevates before serum B12 drops significantly, enabling earlier intervention for athletes experiencing unexplained performance declines or persistent fatigue.
Genetic Factors and Rare Conditions
While B12 deficiency causes most MMA elevations, rare genetic conditions affecting MMA metabolism can also raise levels. Methylmalonic acidemia represents a group of inherited disorders where MMA accumulates regardless of B12 status.
These conditions typically present in infancy or early childhood with severe symptoms including developmental delays, metabolic crisis, and failure to thrive. However, milder variants occasionally present later in life, requiring specialized genetic testing to differentiate from B12 deficiency.
Clinical research on diagnostic accuracy highlights the importance of considering these alternative explanations when MMA remains elevated despite adequate B12 replacement therapy.
Integrating MMA Testing into Preventive Health
Proactive health management increasingly incorporates functional markers like MMA rather than waiting for obvious deficiency symptoms. This preventive approach offers several advantages over reactive testing triggered by clinical problems.
Risk-Based Screening Recommendations
Professional medical organizations recommend B12 screening for high-risk populations, though specific MMA testing guidelines vary. Consider MMA testing if you:
- Follow strict vegetarian or vegan diets for over one year
- Take metformin, proton pump inhibitors, or other interfering medications long-term
- Have digestive conditions affecting nutrient absorption
- Experience unexplained neurological symptoms
- Are over 60 years old with memory concerns
- Have a family history of pernicious anemia
Baseline MMA testing establishes individual reference points for future comparison, making subtle changes easier to detect and address promptly.
Frequency of Repeat Testing
Testing frequency depends on risk factors and previous results:
| Risk Category | Initial Testing | Follow-Up Frequency |
|---|---|---|
| Low risk, normal results | Baseline only | Every 3-5 years |
| High risk, normal results | Annual | Every 6-12 months |
| Borderline elevation | Immediate | Every 3-6 months |
| Confirmed deficiency | During treatment | Per protocol above |
This structured approach balances early detection benefits against unnecessary testing costs and inconvenience.
Understanding the connection between methylmalonic acid and b12 deficiency empowers patients to seek appropriate testing and treatment before irreversible complications develop. MMA testing provides functional assessment of B12 status that standard serum tests cannot deliver, particularly valuable for high-risk populations and those with unexplained symptoms. Whether you're managing known risk factors or investigating concerning symptoms, accessible testing options remove traditional barriers to diagnostic clarity. Justlabs offers convenient, affordable MMA testing with transparent pricing and rapid results, enabling you to take control of your health without the delays and complexity of traditional healthcare channels.