Polycystic Ovary Syndrome (PCOS) affects approximately 10% of women of reproductive age, yet diagnosis remains challenging due to the condition's varied presentation. Many women experience years of frustrating symptoms before receiving a proper diagnosis, often because the right laboratory tests weren't ordered. Understanding which pcos lab tests are essential for diagnosis can help you advocate for comprehensive testing and ensure you receive accurate results that guide effective treatment decisions.
Understanding PCOS: Why Comprehensive Testing Matters
PCOS is not a one-size-fits-all condition. The syndrome manifests through a constellation of symptoms including irregular periods, excess androgen production, insulin resistance, and metabolic dysfunction. Because these symptoms overlap with other endocrine disorders, comprehensive laboratory testing becomes critical for accurate diagnosis.
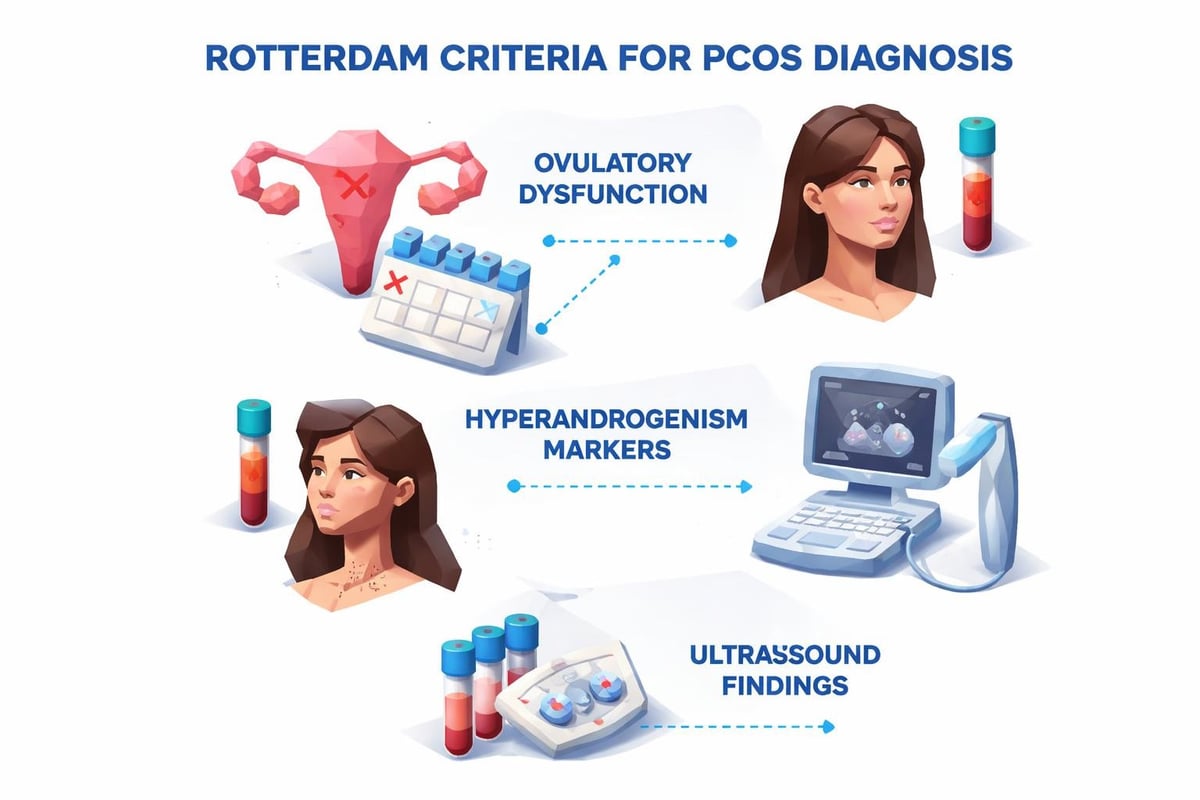
The Rotterdam criteria, widely accepted for PCOS diagnosis, requires meeting two of three conditions: irregular ovulation, clinical or biochemical signs of hyperandrogenism, and polycystic ovaries on ultrasound. Laboratory testing provides the objective data needed to confirm biochemical hyperandrogenism and assess metabolic complications.
Without proper testing, women may receive inappropriate treatments or miss opportunities for early intervention. The right panel of pcos lab tests not only confirms diagnosis but also identifies comorbidities like insulin resistance, thyroid dysfunction, and cardiovascular risk factors that frequently accompany PCOS.
Essential Androgen Tests for PCOS Diagnosis
Hyperandrogenism represents the hallmark biochemical feature of PCOS. Recommended laboratory tests for PCOS diagnosis emphasize measuring multiple androgen markers for comprehensive assessment.
Total Testosterone
Total testosterone serves as the primary screening test for androgen excess. Women with PCOS typically show elevated levels, though values often remain within or just above the normal reference range.
Key considerations for total testosterone testing:
- Morning collection between 8-10 AM ensures accurate results due to diurnal variation
- Mass spectrometry (LC-MS/MS) provides superior accuracy compared to immunoassays
- Levels above 50 ng/dL warrant further investigation for PCOS
- Extremely elevated levels (>150 ng/dL) suggest androgen-secreting tumors requiring additional workup
Free Testosterone and Free Androgen Index
Free testosterone represents the biologically active hormone fraction and often shows abnormalities when total testosterone appears normal. The free androgen index (FAI) calculates the ratio of total testosterone to sex hormone-binding globulin (SHBG), providing an indirect measure of free testosterone.
| Test | Purpose | PCOS Significance |
|---|---|---|
| Free Testosterone | Measures unbound, active testosterone | Often elevated when total testosterone is normal |
| SHBG | Binds sex hormones, reducing bioavailability | Typically decreased in PCOS and insulin resistance |
| Free Androgen Index | Calculated ratio (Total T/SHBG × 100) | Sensitive marker for hyperandrogenism |
Women with PCOS frequently demonstrate low SHBG levels due to insulin resistance, which increases free testosterone availability even when total testosterone remains normal. This relationship makes SHBG measurement essential within comprehensive pcos lab tests.
Recommended Panel
Female Hormone Panel
Save $10This comprehensive panel measures all major female hormones: estrogen, progesterone, reproductive hormones (FSH/LH), and androgens (testosterone/DHEA-S) - essential for understanding hormonal balance.
Includes 7 biomarkers
$89
DHEA-S and Additional Androgens
Dehydroepiandrosterone sulfate (DHEA-S) originates primarily from the adrenal glands. While not specific to PCOS, elevated DHEA-S helps differentiate adrenal from ovarian androgen excess.
Androstenedione, another androgen precursor, may also be measured in comprehensive panels. However, evidence-based laboratory panels for PCOS prioritize testosterone measurements as first-line assessments.
Reproductive Hormone Assessment
Beyond androgens, evaluating reproductive hormones provides insight into ovulatory function and helps exclude other endocrine disorders.
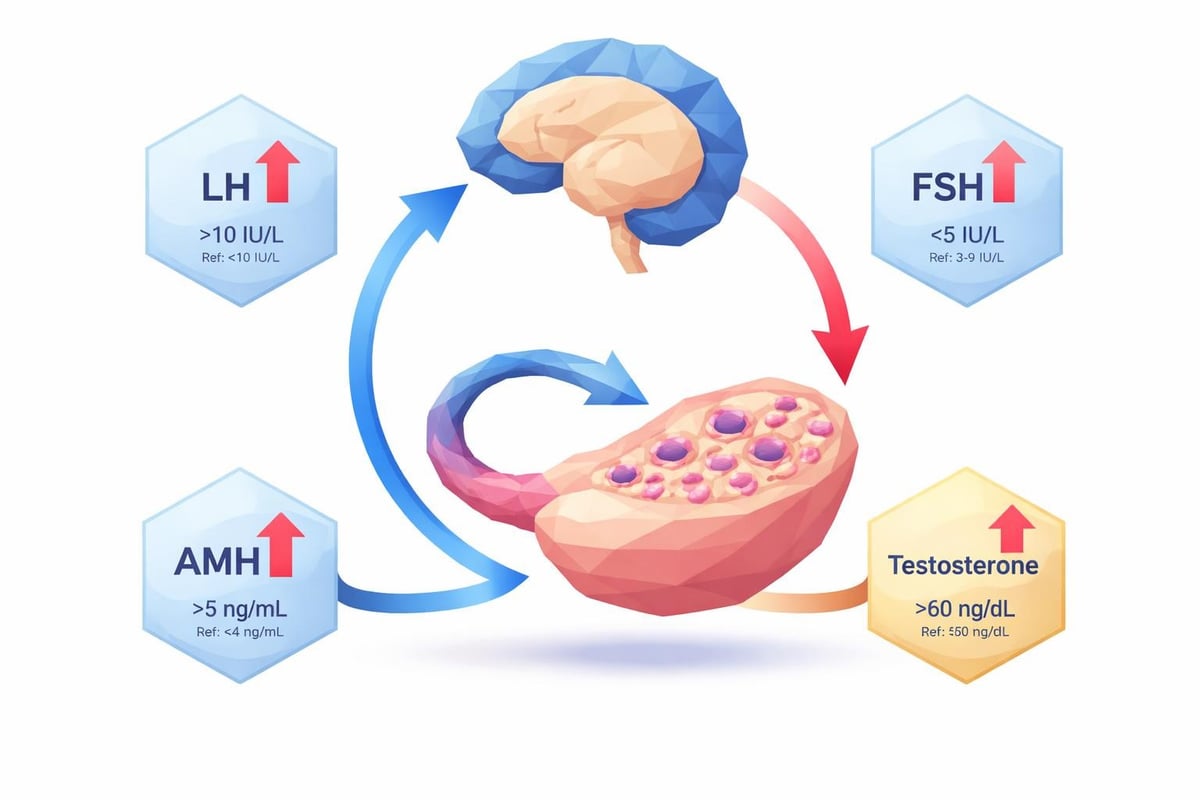
LH and FSH Ratio
Luteinizing hormone (LH) and follicle-stimulating hormone (FSH) regulate ovarian function. Women with PCOS often display an elevated LH to FSH ratio, typically greater than 2:1, though this finding is not universal.
Clinical significance:
- Elevated LH contributes to increased androgen production
- The LH:FSH ratio helps distinguish PCOS from hypothalamic amenorrhea
- Testing should occur during the follicular phase (days 2-5 of cycle)
- Normal ratios do not exclude PCOS diagnosis
Prolactin
Prolactin elevation causes menstrual irregularities and anovulation that mimic PCOS. Testing prolactin levels helps rule out hyperprolactinemia as an alternative diagnosis. Mild elevations may occur with PCOS, while significantly elevated levels suggest a pituitary adenoma requiring imaging studies.
Anti-Müllerian Hormone (AMH)
AMH reflects ovarian follicle count and often shows marked elevation in PCOS. While not required for diagnosis, AMH levels correlate with polycystic ovarian morphology and may provide additional diagnostic information when ultrasound is unavailable or inconclusive.
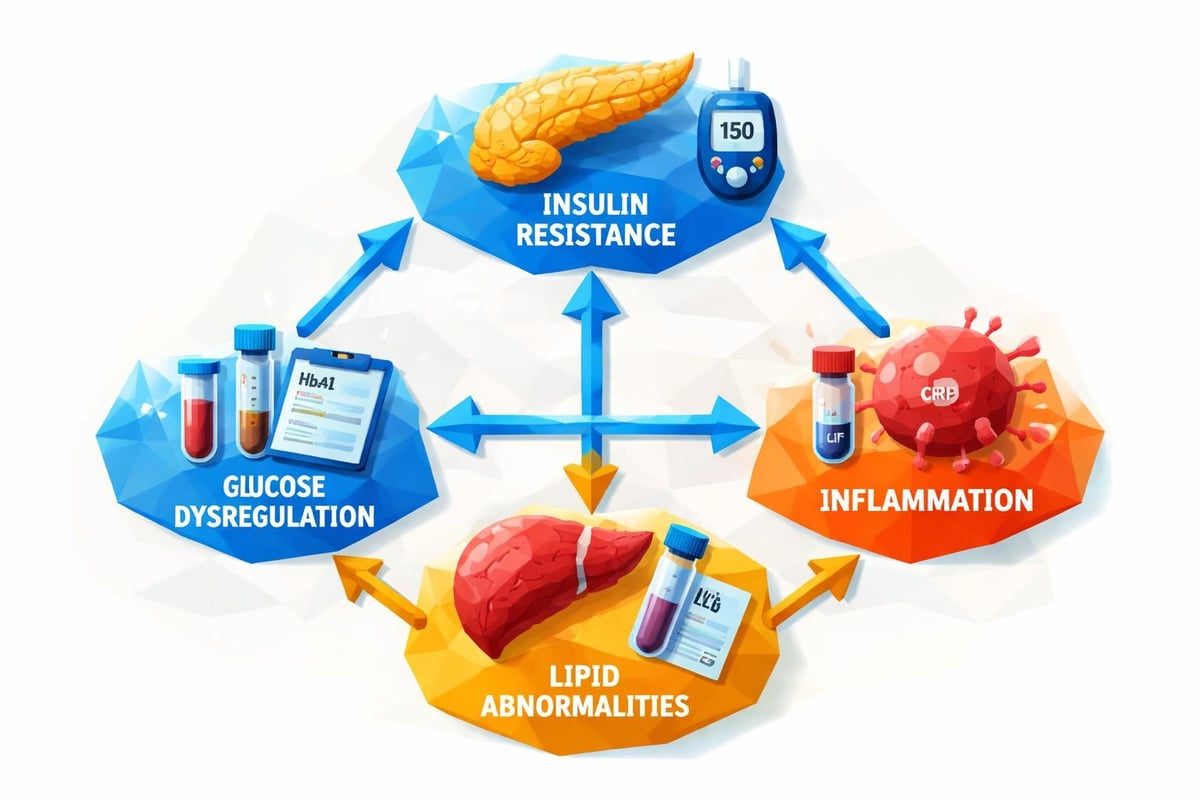
Metabolic Testing: Insulin Resistance and Glucose Dysregulation
Up to 70% of women with PCOS demonstrate insulin resistance, regardless of body weight. Comprehensive diagnostic approaches for PCOS emphasize metabolic screening as critical for long-term health management.
Fasting Glucose and Hemoglobin A1C
Fasting glucose provides a snapshot of current blood sugar levels, while hemoglobin A1C reflects average glucose control over the preceding three months. These tests screen for prediabetes and type 2 diabetes.
Women with PCOS face significantly increased diabetes risk:
- Baseline fasting glucose and A1C establish metabolic status
- Values in the prediabetic range warrant aggressive lifestyle intervention
- Regular monitoring every 1-2 years helps detect progression
- Early detection enables preventive treatment before diabetes develops
Insulin Testing and HOMA-IR
Fasting insulin levels and the homeostatic model assessment of insulin resistance (HOMA-IR) quantify insulin resistance severity. HOMA-IR calculates using fasting glucose and insulin values, with scores above 2.5 indicating significant insulin resistance.
Direct insulin measurement offers advantages over glucose testing alone, as insulin resistance develops years before fasting glucose becomes abnormal. Many women with PCOS and normal glucose show markedly elevated insulin levels.
Recommended Panel
Complete Metabolic Health Panel
Save $3.5This comprehensive panel evaluates all aspects of metabolic health: organ function, cholesterol, blood sugar, insulin resistance, and inflammation - the key drivers of chronic disease.
Includes 26 biomarkers
$50
Fasting required
Oral Glucose Tolerance Test
The two-hour oral glucose tolerance test (OGTT) remains the gold standard for detecting glucose dysregulation. This test involves measuring glucose (and optionally insulin) at baseline and two hours after consuming a 75-gram glucose solution.
The OGTT identifies impaired glucose tolerance missed by fasting tests alone. Some clinicians measure insulin at multiple timepoints during the OGTT to assess insulin response patterns, though this remains controversial regarding clinical utility versus cost.
Lipid Profile and Cardiovascular Risk Assessment
PCOS increases cardiovascular disease risk through multiple mechanisms including dyslipidemia, hypertension, and chronic inflammation. A comprehensive lipid panel evaluates cardiovascular risk factors.
Standard lipid panel components:
- Total cholesterol
- LDL cholesterol (low-density lipoprotein)
- HDL cholesterol (high-density lipoprotein)
- Triglycerides
- Non-HDL cholesterol (calculated)
Women with PCOS frequently show characteristic lipid abnormalities including elevated triglycerides, reduced HDL cholesterol, and increased small, dense LDL particles. These patterns indicate increased cardiovascular risk requiring monitoring and potential intervention.
Advanced lipid testing may include apolipoprotein B (ApoB), lipoprotein(a), and particle size analysis for comprehensive cardiovascular risk stratification, particularly in women with family history of early heart disease.
Thyroid Function Testing
Thyroid disorders occur more frequently in women with PCOS than in the general population. Hypothyroidism causes symptoms overlapping with PCOS, including menstrual irregularities, weight gain, and metabolic dysfunction.
TSH and Free T4
Thyroid-stimulating hormone (TSH) serves as the primary thyroid screening test. Abnormal TSH warrants measurement of free thyroxine (free T4) to assess thyroid hormone production.
| Condition | TSH | Free T4 | Clinical Significance |
|---|---|---|---|
| Primary Hypothyroidism | Elevated | Low or normal | Most common thyroid disorder in PCOS |
| Subclinical Hypothyroidism | Mildly elevated | Normal | May worsen PCOS symptoms and fertility |
| Hyperthyroidism | Suppressed | Elevated | Rare, but causes menstrual irregularities |
Subclinical hypothyroidism, characterized by elevated TSH with normal free T4, affects approximately 15-20% of women with PCOS. Treatment remains controversial but may improve metabolic parameters and fertility outcomes.
Recommended Panel
Basic Thyroid Panel
Save $2This panel includes the 3 essential thyroid markers: TSH, Free T4, and Free T3. The perfect starting point for evaluating thyroid function without unnecessary tests.
Includes 3 biomarkers
$30
Thyroid Antibodies
Testing for thyroid peroxidase (TPO) antibodies and thyroglobulin antibodies identifies autoimmune thyroid disease. Hashimoto's thyroiditis frequently coexists with PCOS, and positive antibodies predict progression to overt hypothyroidism requiring monitoring and potential treatment.
Additional Diagnostic Tests to Consider
Depending on individual presentation and risk factors, additional pcos lab tests may provide valuable diagnostic information.
17-Hydroxyprogesterone
Early morning 17-hydroxyprogesterone (17-OHP) screening helps exclude non-classical congenital adrenal hyperplasia (NCAH), which mimics PCOS. Mildly elevated values require ACTH stimulation testing for definitive diagnosis. Laboratory tests used to diagnose PCOS should include 17-OHP in women with significant hyperandrogenism.
Vitamin D
Vitamin D deficiency appears more prevalent in women with PCOS and correlates with insulin resistance severity. While not diagnostic, vitamin D measurement identifies a modifiable factor potentially improving metabolic and reproductive outcomes through supplementation.
High-Sensitivity C-Reactive Protein
hs-CRP measures systemic inflammation, which contributes to cardiovascular risk in PCOS. Elevated levels indicate increased risk and may prompt more aggressive cardiovascular risk reduction strategies.
Complete Blood Count and Liver Function
Basic screening with complete blood count (CBC) and comprehensive metabolic panel (CMP) establishes baseline health status and identifies common issues like anemia or liver enzyme elevations related to fatty liver disease, which occurs frequently with insulin resistance.
Timing and Preparation for PCOS Lab Tests
Proper timing and preparation ensure accurate results. Most pcos lab tests require specific conditions for optimal interpretation.
Testing guidelines:
- Fasting requirements: Most metabolic tests require 8-12 hours of fasting, including glucose, insulin, and lipid panels
- Timing within menstrual cycle: Reproductive hormones should be measured on days 2-5 of the menstrual cycle when possible
- Morning collection: Testosterone, cortisol, and other hormones require morning collection (8-10 AM) due to diurnal variation
- Medication considerations: Inform the laboratory about hormonal contraceptives, metformin, or other medications affecting hormone levels
Women with irregular cycles or amenorrhea face challenges regarding cycle timing. Ordering lab tests without a doctor through services like Justlabs provides flexibility in timing, though consultation regarding optimal scheduling remains important for accurate interpretation.
Interpreting Your PCOS Lab Test Results
Understanding laboratory results requires context. Reference ranges vary between laboratories, and "normal" ranges may not represent optimal values for women with PCOS.
Working with Reference Ranges
Laboratory reference ranges typically represent the middle 95% of the population. However, women with PCOS may show abnormalities within the normal range or borderline elevations that hold clinical significance.
For example, total testosterone of 45 ng/dL falls within many laboratories' normal range (typically 15-70 ng/dL) but represents the upper end of normal, particularly when combined with low SHBG and elevated free testosterone. Understanding lab results helps identify patterns suggesting PCOS even when individual values remain technically normal.
Recognizing Patterns
PCOS diagnosis relies on patterns rather than individual abnormal values. The combination of findings provides diagnostic clarity:
- Elevated testosterone with low SHBG and elevated free androgen index
- Elevated LH:FSH ratio with irregular cycles
- Elevated insulin with normal fasting glucose
- Dyslipidemia with markers of insulin resistance
Single abnormal values require confirmation and clinical correlation. Multiple consistent abnormalities strengthen diagnostic confidence.
Cost Considerations and Access to Testing
Traditional diagnostic workups for PCOS can become expensive, particularly without insurance coverage or with high-deductible plans. Individual tests range from $30-$200 or more depending on the specific marker and testing method.
Comprehensive pcos lab tests panels may include 10-15 different markers, creating significant out-of-pocket costs. However, self-pay laboratory services provide transparent pricing and often cost less than insurance-based testing after deductibles and copays.
Cost-saving strategies include:
- Prioritizing essential tests (androgens, glucose/insulin, TSH) before additional markers
- Using direct-to-consumer laboratory services with published pricing
- Spacing tests appropriately rather than repeating unnecessarily
- Comparing costs between traditional healthcare systems and self-pay options
Access to testing without requiring physician orders allows women to pursue comprehensive evaluation when doctors dismiss symptoms or order inadequate panels. How lab testing works through direct access services empowers patients to advocate for thorough evaluation.
Monitoring and Follow-Up Testing
Initial diagnosis represents just the beginning. PCOS requires ongoing monitoring to assess treatment effectiveness and screen for developing complications.
Treatment Response Monitoring
After initiating treatment (lifestyle modifications, metformin, hormonal contraceptives, or other interventions), repeat testing evaluates response:
- Metabolic markers every 3-6 months initially, then annually
- Androgen levels if hirsutism or acne remains problematic
- A1C every 3-6 months with prediabetes or during weight loss interventions
- Lipid panel annually or more frequently with abnormal values
Long-Term Surveillance
Even with well-controlled PCOS, long-term surveillance identifies emerging issues:
- Annual metabolic screening (glucose, A1C, lipids) detects diabetes risk progression
- Periodic thyroid testing every 1-2 years monitors for developing hypothyroidism
- Cardiovascular risk assessment guides preventive interventions
- Fertility monitoring when pregnancy planning becomes relevant
Consistent monitoring enables proactive management, preventing complications before they develop. Affordable and transparent pricing makes regular surveillance feasible without insurance barriers or surprise bills.
Common Testing Mistakes to Avoid
Several common errors compromise diagnostic accuracy or lead to unnecessary testing.
Avoid these mistakes:
- Testing during hormonal contraceptive use, which suppresses natural hormone production
- Random timing without considering menstrual cycle phase
- Skipping fasting requirements for metabolic tests
- Accepting incomplete panels that miss important markers
- Failing to confirm abnormal results before starting treatment
- Over-testing with unnecessary markers that don't influence management
Quality matters more than quantity. A focused panel of essential pcos lab tests performed correctly provides more value than extensive testing done improperly.
When to Seek Additional Evaluation
While pcos lab tests confirm most diagnoses, certain findings warrant additional investigation:
- Extremely elevated testosterone (>150 ng/dL) suggesting androgen-secreting tumor
- Markedly elevated DHEA-S indicating adrenal pathology
- Abnormal thyroid function requiring endocrinology referral
- Significantly elevated prolactin necessitating pituitary imaging
- Cushingoid features suggesting Cushing's syndrome
These situations require specialist evaluation beyond standard PCOS workup. Don't hesitate to pursue additional testing when initial results suggest alternative or additional diagnoses.
Comprehensive pcos lab tests provide the foundation for accurate diagnosis and effective treatment of this complex endocrine disorder. Understanding which tests to request, how to prepare properly, and how to interpret results empowers women to advocate for thorough evaluation and appropriate care. Whether you're experiencing symptoms requiring initial workup or need ongoing monitoring of established PCOS, Justlabs offers convenient access to comprehensive testing with transparent pricing and rapid results, helping you take control of your health without the barriers of traditional healthcare systems.


