If you've been tossing and turning night after night, you might assume insomnia is purely psychological or stress-related. However, many cases of persistent sleep problems stem from measurable deficiencies and imbalances that can be identified through specific laboratory tests. Understanding which lab tests for insomnia can reveal underlying causes like iron deficiency, magnesium depletion, or cortisol dysregulation gives you actionable data to address your sleep problems at their root.
Why Laboratory Testing Matters for Persistent Insomnia
Sleep difficulties affect millions of Americans, but not all insomnia has the same cause. While diagnosing insomnia typically begins with evaluating sleep patterns and medical history, many healthcare providers overlook the biochemical factors that sabotage sleep quality.
Laboratory testing provides objective measurements that can identify:
- Nutritional deficiencies affecting neurotransmitter production
- Hormonal imbalances disrupting circadian rhythms
- Inflammatory markers indicating systemic issues
- Metabolic dysfunction interfering with sleep regulation
Unlike subjective sleep diaries or questionnaires, lab tests for insomnia deliver quantifiable data. This precision allows for targeted interventions rather than generic sleep hygiene recommendations that may not address your specific problem.
The Self-Pay Testing Advantage
Traditional insomnia evaluations through insurance often require multiple doctor visits, referrals, and weeks of waiting. Modern self-pay testing services streamline this process significantly. When you order labs without a doctor, you gain immediate access to the specific tests that matter most for your situation.
The cost transparency and speed of self-pay options make investigating potential deficiencies practical and affordable. Results typically arrive within 1-3 days, allowing you to move forward with treatment quickly rather than waiting through bureaucratic delays.
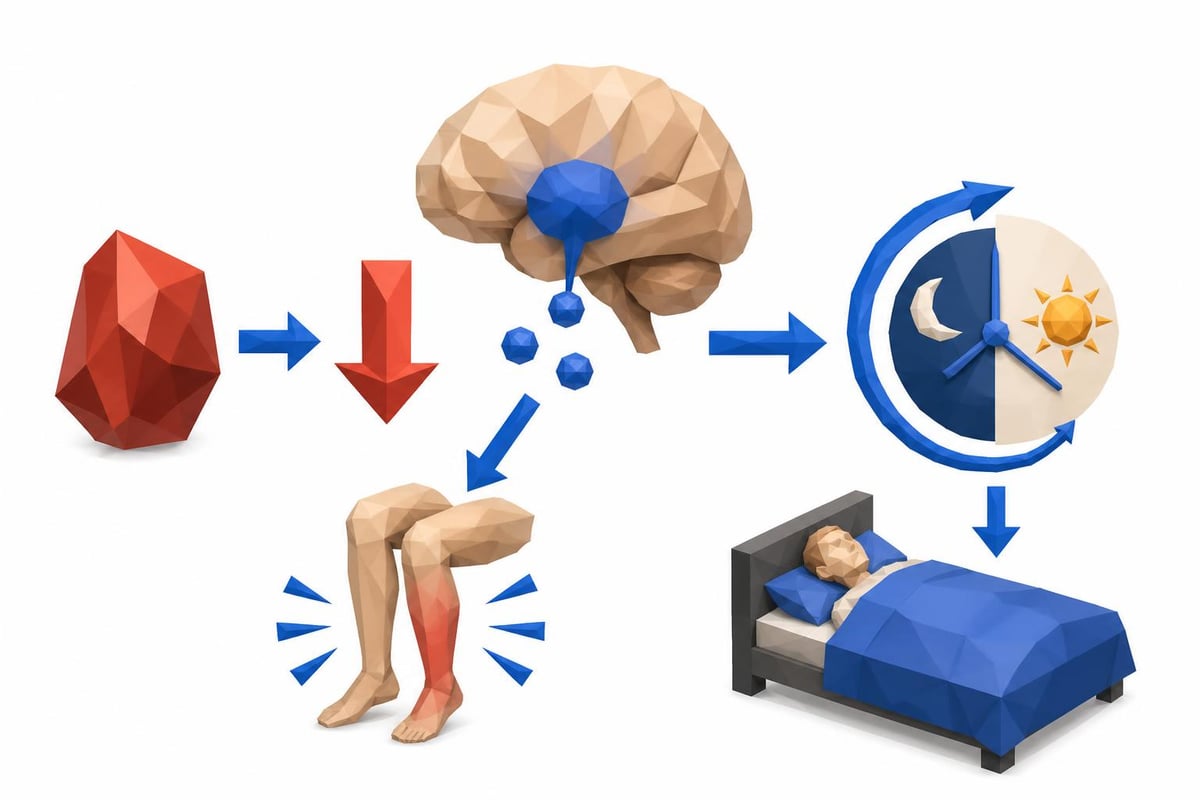
Iron Deficiency: The Hidden Sleep Disruptor
Iron plays a crucial role in sleep regulation that most people never consider. This essential mineral is required for dopamine synthesis, and dopamine directly influences sleep quality and the ability to maintain continuous rest throughout the night.
Low iron levels correlate strongly with several sleep-related conditions:
- Restless leg syndrome (RLS), which prevents sleep onset
- Periodic limb movement disorder during sleep
- Reduced slow-wave sleep duration
- Frequent nighttime awakenings
Research shows that even borderline iron deficiency, which wouldn't necessarily cause anemia, can significantly impact sleep quality. The standard complete blood count (CBC) might show normal hemoglobin while ferritin levels tell a different story.
Essential Iron Tests for Sleep Problems
| Test Name | What It Measures | Optimal Range for Sleep |
|---|---|---|
| Ferritin | Iron storage levels | 50-100 ng/mL |
| Serum Iron | Circulating iron | 60-170 mcg/dL |
| TIBC | Iron-binding capacity | 250-450 mcg/dL |
| Transferrin Saturation | Iron utilization | 20-50% |
Ferritin deserves special attention as the most sensitive early indicator of iron deficiency. Many labs consider ferritin levels above 15 ng/mL as "normal," but for optimal sleep, levels should be substantially higher. Studies on restless leg syndrome show that ferritin below 50 ng/mL commonly triggers symptoms, even when other iron markers appear adequate.
When evaluating lab tests for insomnia, iron panels should be among the first ordered, particularly if you experience leg discomfort or movement urges at night. Women with heavy menstrual periods, vegetarians, and frequent blood donors face higher risk for sleep-disrupting iron deficiency.
Magnesium Deficiency and Sleep Architecture
Magnesium serves as a cofactor in over 300 enzymatic reactions, including those that regulate the neurotransmitters responsible for calming the nervous system. This mineral directly impacts GABA (gamma-aminobutyric acid) activity, which promotes relaxation and sleep onset.
Unfortunately, standard blood tests often miss magnesium deficiency. Serum magnesium represents less than 1% of total body magnesium stores, making it a poor indicator of true deficiency status.
The signs of magnesium deficiency affecting sleep include:
- Difficulty falling asleep despite feeling tired
- Muscle tension and cramping at night
- Anxiety and racing thoughts before bed
- Frequent middle-of-the-night awakening
- Non-restorative sleep despite adequate duration
Magnesium Testing Options
For accurate assessment, consider these lab tests for insomnia related to magnesium status:
RBC Magnesium (Red Blood Cell Magnesium) provides a better picture of intracellular stores compared to serum testing. This test reflects magnesium levels over the previous 120 days, offering a more stable measurement.
Magnesium Loading Test involves measuring urinary magnesium excretion after an oral or intravenous magnesium dose. Retention of more than 20% of the administered dose suggests deficiency, though this test requires more coordination and isn't available through all testing services.
Serum Magnesium, while limited, remains useful when combined with clinical symptoms and other markers. Normal range typically falls between 1.7-2.2 mg/dL, but optimal levels for sleep should be in the upper half of this range.
Dietary surveys suggest that up to 75% of Americans don't meet the recommended daily intake for magnesium. Factors like chronic stress, certain medications (especially proton pump inhibitors), and high calcium intake can further deplete magnesium stores, making deficiency remarkably common among insomnia sufferers.
Recommended Test
Magnesium, RBC
RBC (red blood cell) magnesium measures magnesium inside your cells, providing a more accurate assessment of your true magnesium status than standard serum magnesium tests.
Includes 1 biomarkers
$15
Cortisol Dysregulation: When Your Stress Hormone Runs Wild
Cortisol follows a natural daily rhythm, rising in the early morning to promote wakefulness and declining throughout the day to allow sleep onset. When this pattern becomes disrupted, insomnia often follows. According to Stanford Healthcare's diagnostic guidelines, evaluating the hypothalamic-pituitary-adrenal (HPA) axis can reveal important information about sleep disorders.
Three cortisol patterns commonly interfere with sleep:
- Elevated nighttime cortisol prevents sleep onset and causes middle-of-the-night awakening
- Flat cortisol rhythm with insufficient morning rise and inadequate evening decline
- Reversed cortisol pattern with low morning and high evening levels
Standard cortisol testing typically involves a single morning blood draw, which provides minimal information about daily rhythm. For insomnia evaluation, more comprehensive testing is essential.
Comprehensive Cortisol Testing for Sleep Issues
Cortisol Awakening Response (CAR) testing measures cortisol at awakening and 30-45 minutes later. This captures the natural morning surge, which should show a 50-75% increase. Blunted or absent awakening response correlates with sleep problems and fatigue.
Four-Point Salivary Cortisol testing tracks levels at morning, noon, evening, and bedtime. This captures the full diurnal rhythm and identifies specific patterns affecting sleep. Collection occurs at home, making it convenient and reducing the stress-induced cortisol spike that can occur with blood draws.
24-Hour Urinary Free Cortisol provides an integrated measurement of total cortisol production throughout the day. While it doesn't show timing patterns, it reveals whether overall production is excessive or insufficient.
| Test Type | What It Shows | Best For |
|---|---|---|
| Morning Serum Cortisol | Peak cortisol level | Screening for extremes |
| CAR (saliva) | Awakening response | Chronic fatigue with insomnia |
| 4-Point Salivary | Daily rhythm pattern | Sleep onset and maintenance issues |
| 24-Hour Urine | Total daily production | Overall HPA axis function |
When cortisol remains elevated at bedtime, it directly antagonizes melatonin production and maintains sympathetic nervous system activation. This creates a state of hyperarousal that makes sleep initiation nearly impossible, regardless of sleep hygiene practices.
Recommended Test
Cortisol, Total
Cortisol is your body's primary stress hormone, produced by the adrenal glands. This test measures total cortisol levels to assess adrenal function and stress response.
Includes 1 biomarkers
$15
Thyroid Function and Sleep Quality
Thyroid hormones regulate metabolic rate and affect virtually every system in the body, including sleep architecture. Both hypothyroidism and hyperthyroidism can cause insomnia, though through different mechanisms.
Hypothyroidism (low thyroid function) often causes:
- Difficulty achieving deep sleep stages
- Sleep apnea or breathing irregularities
- Daytime fatigue requiring excessive sleep attempts
- Depression affecting sleep quality
Hyperthyroidism (excessive thyroid function) typically produces:
- Racing thoughts preventing sleep onset
- Anxiety and nighttime restlessness
- Reduced total sleep need with daytime agitation
- Heat intolerance affecting comfort
Complete Thyroid Panel for Sleep Issues
Basic thyroid screening only measures TSH (thyroid-stimulating hormone), which can miss subclinical thyroid dysfunction affecting sleep. A comprehensive evaluation should include:
- TSH: Primary screening marker (optimal range 1.0-2.5 mIU/L for sleep)
- Free T4: Storage form of thyroid hormone
- Free T3: Active thyroid hormone affecting metabolism
- Reverse T3: Inactive form that can block T3 action
- Thyroid antibodies: TPO and thyroglobulin to identify autoimmune thyroid disease
The ratio of Free T3 to Reverse T3 provides insight into cellular thyroid hormone activity. When stress or inflammation is high, the body converts more T4 to Reverse T3 rather than active T3, creating functional hypothyroidism even when standard tests appear normal.
Blood Sugar Regulation and Nighttime Awakening
Middle-of-the-night awakening, particularly between 2-4 AM, frequently results from blood sugar fluctuations. When blood glucose drops too low during sleep, the body releases counter-regulatory hormones (cortisol, adrenaline, glucagon) to raise it back up. This hormonal surge can wake you completely or shift you from deep sleep to light sleep.
Blood sugar-related lab tests for insomnia include:
- Fasting Glucose: Should be 70-85 mg/dL (optimal) rather than just under 100 mg/dL
- Hemoglobin A1c: Reflects 3-month average glucose; optimal is 4.8-5.2%
- Fasting Insulin: Measures insulin resistance; optimal is under 5 mIU/L
- HOMA-IR: Calculated insulin resistance score; under 1.0 is ideal
The combination of fasting glucose and fasting insulin provides the most information about metabolic health affecting sleep. You can have "normal" fasting glucose while insulin is already elevated, indicating insulin resistance that disrupts sleep through multiple pathways.
Reactive hypoglycemia, where blood sugar drops sharply 2-4 hours after eating, particularly affects evening meals that precede bedtime. This creates middle-of-the-night crashes that fragment sleep through hormonal activation.
Vitamin D and Sleep Regulation
Vitamin D receptors exist throughout the brain, including regions that regulate sleep. Research links vitamin D deficiency to shorter sleep duration, poor sleep quality, and daytime sleepiness. The mechanisms involve vitamin D's role in neurotransmitter production and circadian rhythm regulation.
Testing considerations for vitamin D:
Testing serum 25-hydroxyvitamin D [25(OH)D] provides the standard measurement. While labs typically classify levels above 30 ng/mL as sufficient, research on sleep quality suggests optimal levels between 50-70 ng/mL.
Vitamin D deficiency is extremely prevalent, particularly in northern latitudes, during winter months, and among people with darker skin or limited sun exposure. According to research on laboratory testing strategies, selective testing based on risk factors provides the most cost-effective approach.
Recommended Test
Vitamin D, 25-Hydroxy
Vitamin D deficiency affects over 40% of Americans. This test measures your vitamin D status, essential for bone health, immune function, mood, and much more.
Includes 2 biomarkers
$25
When to Consider Lab Tests for Insomnia
Not everyone with occasional sleep difficulty needs extensive laboratory testing. However, certain situations strongly indicate that lab work could identify treatable causes.
Consider testing if you experience:
- Insomnia persisting longer than 3 months despite sleep hygiene improvements
- Specific symptoms suggesting deficiency (restless legs, muscle cramps, anxiety)
- Medical conditions associated with nutritional deficiencies (celiac disease, gastric bypass)
- Medications that deplete specific nutrients (metformin affects B12, statins affect CoQ10)
- High stress levels suggesting HPA axis dysregulation
The Sleep Foundation's diagnostic criteria emphasize that testing should complement, not replace, a thorough sleep history and evaluation of sleep habits. Laboratory tests reveal what's happening biochemically but require clinical context for proper interpretation.
Creating Your Testing Strategy
Rather than ordering every possible test, prioritize based on your specific symptoms and risk factors. A strategic approach might look like this:
Tier 1 Testing (Most Common Deficiencies):
- Complete blood count with ferritin
- Comprehensive metabolic panel
- TSH and Free T4
- Vitamin D 25-hydroxyvitamin D
Tier 2 Testing (Based on Tier 1 Results and Symptoms):
- RBC magnesium
- Free T3 and Reverse T3
- Fasting insulin and glucose
- Four-point salivary cortisol
Tier 3 Testing (Specialized Evaluation):
- Sleep study (polysomnography) if sleep apnea suspected
- Comprehensive hormone panel
- Inflammatory markers (hsCRP, homocysteine)
- Nutrient panels for B vitamins, zinc, copper
Understanding how lab test pricing works helps you budget for comprehensive evaluation without surprise costs. Transparent pricing allows you to select the most relevant tests for your situation.
Interpreting Results and Next Steps
Laboratory tests provide data points, but optimal ranges for sleep often differ from standard reference ranges designed to identify disease. A result classified as "normal" by the lab might still be suboptimal for sleep quality.
Work with these interpretation principles:
- Consider symptoms alongside numbers (symptomatic low-normal is still significant)
- Understand that reference ranges represent population averages, not optimal health
- Look for patterns across multiple related markers
- Retest after interventions to confirm improvement
For example, ferritin at 20 ng/mL is technically "normal" but commonly causes restless leg syndrome and poor sleep. Supplementation to raise ferritin above 50 ng/mL often resolves sleep issues completely, despite the original level not being classified as deficient.
When deficiencies are identified, correction timelines vary. Iron repletion may take 3-6 months. Magnesium improves more quickly, often within 2-4 weeks. Thyroid optimization requires careful dose adjustments over several months. Cortisol rhythm restoration through stress management and circadian rhythm practices can take 6-12 months.
The Role of Inflammation in Sleep Disruption
Chronic low-grade inflammation affects sleep through multiple pathways, including cytokine production that influences sleep architecture. While not always considered in standard insomnia workups, inflammatory markers can provide valuable information.
Key inflammatory markers affecting sleep:
- High-sensitivity C-Reactive Protein (hsCRP): Should be under 1.0 mg/L for optimal health
- Homocysteine: Elevated levels indicate methylation problems affecting neurotransmitters
- Erythrocyte Sedimentation Rate (ESR): General inflammation marker
Inflammation disrupts sleep by increasing pro-inflammatory cytokines like IL-6 and TNF-alpha, which interfere with normal sleep regulation. These same cytokines can cause daytime fatigue despite inadequate nighttime sleep, creating a frustrating cycle.
Identifying inflammation sources, whether from gut dysfunction, chronic infections, autoimmune conditions, or metabolic syndrome, allows targeted treatment that often improves sleep as a secondary benefit.
Identifying the specific deficiencies disrupting your sleep through targeted laboratory testing removes the guesswork from insomnia treatment. Rather than trying random supplements or accepting poor sleep as inevitable, lab tests for insomnia provide concrete data about iron, magnesium, cortisol, and other biochemical factors affecting your rest. When you're ready to investigate the root causes of your sleep problems with affordable, accessible testing, Justlabs offers a straightforward path to answers, with transparent pricing and results delivered in 1-3 days so you can start addressing your sleep issues quickly.