Understanding the connection between elevated ferritin levels and genetic conditions requires careful evaluation of multiple iron markers. When ferritin rises significantly without obvious causes like inflammation or liver disease, genetic iron overload becomes a critical consideration. The relationship between high ferritin genetic iron TIBC measurements reveals important information about hereditary hemochromatosis, a condition where the body absorbs and stores excessive iron due to inherited mutations. This comprehensive evaluation combines ferritin, serum iron, and total iron-binding capacity (TIBC) to distinguish genetic iron overload from other conditions that elevate ferritin levels.
The Biology Behind High Ferritin Genetic Iron TIBC Patterns
Iron metabolism involves a complex regulatory system that balances absorption, storage, and utilization. Ferritin serves as the primary storage protein for iron, while serum iron measures the amount circulating in the bloodstream. TIBC reflects transferrin's capacity to bind and transport iron throughout the body.
In genetic iron overload conditions, specific patterns emerge that distinguish hereditary causes from acquired conditions. When hemochromatosis is present, the body continuously absorbs excess dietary iron regardless of actual storage levels. This inappropriate absorption stems from mutations in genes responsible for regulating iron homeostasis.
Key Markers in Iron Overload Assessment
The iron panel evaluation includes:
- Serum ferritin: Reflects total body iron stores
- Serum iron: Measures iron currently in circulation
- TIBC: Indicates transferrin's binding capacity
- Transferrin saturation: Calculated percentage showing how saturated transferrin is with iron
The transferrin saturation percentage provides particularly valuable diagnostic information. This calculation divides serum iron by TIBC, then multiplies by 100. In hereditary hemochromatosis, transferrin saturation typically exceeds 45% in affected individuals, often reaching 60-90% in severe cases.

Normal iron regulation depends on hepcidin, a hormone produced by the liver that controls iron absorption in the intestines. Hereditary hyperferritinemia results from genetic mutations that impair hepcidin production or function, allowing unchecked iron absorption even when stores are already elevated.
Genetic Causes of Elevated Ferritin and Iron
Hereditary hemochromatosis represents the most common genetic cause of iron overload in populations of Northern European descent. Multiple genetic mutations can produce this condition, with varying severity and inheritance patterns.
HFE-Related Hemochromatosis
The HFE gene mutations account for approximately 85-90% of hereditary hemochromatosis cases. Two primary mutations deserve attention: C282Y and H63D. The C282Y homozygous genotype (two copies of the mutation) produces the most significant iron overload risk.
Individuals with two C282Y mutations demonstrate classic high ferritin genetic iron TIBC patterns. Their transferrin saturation rises early, often during young adulthood, followed by progressive ferritin elevation. Without intervention, iron accumulates in the liver, heart, pancreas, and joints, potentially causing organ damage.
Compound heterozygotes carrying one C282Y and one H63D mutation show milder iron loading. Many never develop clinically significant overload, though monitoring remains important. H63D homozygotes rarely demonstrate severe iron accumulation.
| Genotype | Risk Level | Typical Ferritin Pattern | Clinical Significance |
|---|---|---|---|
| C282Y/C282Y | High | Progressive elevation | Requires treatment |
| C282Y/H63D | Moderate | Variable elevation | Monitor regularly |
| H63D/H63D | Low | Usually normal | Minimal risk |
| C282Y/wild-type | Low | Usually normal | Carrier status |
Non-HFE Hemochromatosis Variants
Several rarer genetic forms produce severe iron overload, often presenting earlier than HFE-related disease. These conditions involve different genes in the iron regulation pathway but produce similar high ferritin genetic iron TIBC abnormalities.
Juvenile hemochromatosis results from mutations in either the HJV or HAMP genes. These conditions cause severe iron accumulation beginning in the teenage years or early twenties. Affected individuals may develop heart disease and endocrine dysfunction before age 30 without early diagnosis and treatment.
Ferroportin disease stems from mutations in the SLC40A1 gene, producing two distinct patterns. Type A causes iron accumulation primarily in macrophages, while Type B resembles classic hemochromatosis with hepatocyte iron loading.
Transferrin receptor 2 mutations produce hemochromatosis similar to HFE-related disease but typically with earlier onset and more aggressive progression.
Diagnostic Approach to High Ferritin Genetic Iron TIBC
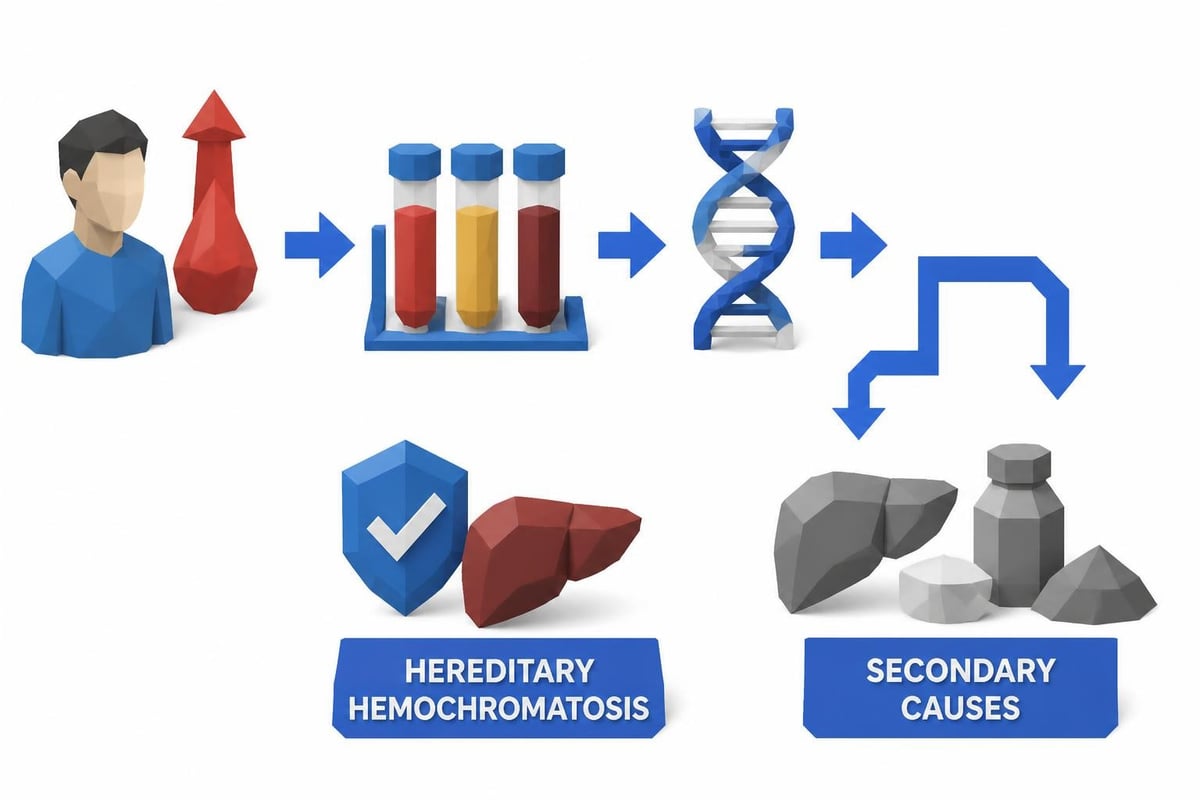
Evaluating elevated ferritin requires systematic investigation to distinguish genetic causes from secondary conditions. Many factors elevate ferritin without true iron overload, including inflammation, infection, liver disease, metabolic syndrome, and malignancy.
Investigating elevated serum ferritin begins with measuring the complete iron panel. When transferrin saturation exceeds 45% along with elevated ferritin, genetic testing becomes appropriate. However, interpretation requires careful consideration of clinical context.
Testing Sequence for Suspected Genetic Iron Overload
- Initial screening: Measure fasting transferrin saturation and serum ferritin
- Confirm abnormalities: Repeat testing to verify persistent elevation
- Assess inflammation: Check C-reactive protein to exclude inflammatory ferritin elevation
- Genetic testing: Analyze HFE mutations (C282Y and H63D) as first-line genetic evaluation
- Advanced testing: Consider non-HFE genetic testing if HFE negative with strong clinical suspicion
The Province of British Columbia's iron overload guidelines provide comprehensive diagnostic algorithms. These protocols help clinicians navigate the evaluation process efficiently while avoiding unnecessary testing.
Interpreting Results in Context
Transferrin saturation provides the earliest indicator of genetic iron overload, often rising years before ferritin becomes significantly elevated. In early hemochromatosis, individuals may demonstrate transferrin saturation above 60% while ferritin remains under 300 ng/mL.
TIBC typically decreases in iron overload because transferrin becomes saturated with iron, reducing the total binding capacity. This contrasts with iron deficiency, where TIBC rises as the body attempts to capture more dietary iron.
When evaluating high ferritin genetic iron TIBC patterns, consider these reference ranges:
- Normal ferritin: 30-200 ng/mL (men), 15-150 ng/mL (women)
- Normal serum iron: 60-170 mcg/dL
- Normal TIBC: 250-450 mcg/dL
- Normal transferrin saturation: 20-50%
Understanding Metabolic Hyperferritinaemia
Not all genetic conditions affecting ferritin involve true iron overload. Metabolic hyperferritinaemia represents a distinct entity where ferritin rises in association with insulin resistance and metabolic syndrome, even without excessive iron stores.
This condition blurs the lines between genetic predisposition and acquired metabolic dysfunction. Individuals with metabolic syndrome often demonstrate elevated ferritin with normal or only mildly elevated transferrin saturation. The ferritin elevation reflects inflammation and altered iron metabolism rather than true overload.
Distinguishing Features
| Feature | Hereditary Hemochromatosis | Metabolic Hyperferritinaemia |
|---|---|---|
| Transferrin saturation | >45%, often >60% | Usually <45% |
| Iron stores (MRI/biopsy) | Markedly elevated | Normal to mildly elevated |
| Response to phlebotomy | Sustained improvement | Limited benefit |
| Associated conditions | Genetic mutations | Metabolic syndrome, NAFLD |
Genetic factors influence metabolic hyperferritinaemia susceptibility, though not through classic hemochromatosis mutations. Polymorphisms affecting inflammation, insulin signaling, and lipid metabolism contribute to this phenotype.
Management Strategies for Genetic Iron Overload
Early detection and treatment prevent complications from hereditary hemochromatosis. Once diagnosis confirms genetic iron overload through high ferritin genetic iron TIBC patterns and positive genetic testing, therapeutic phlebotomy becomes the primary treatment.
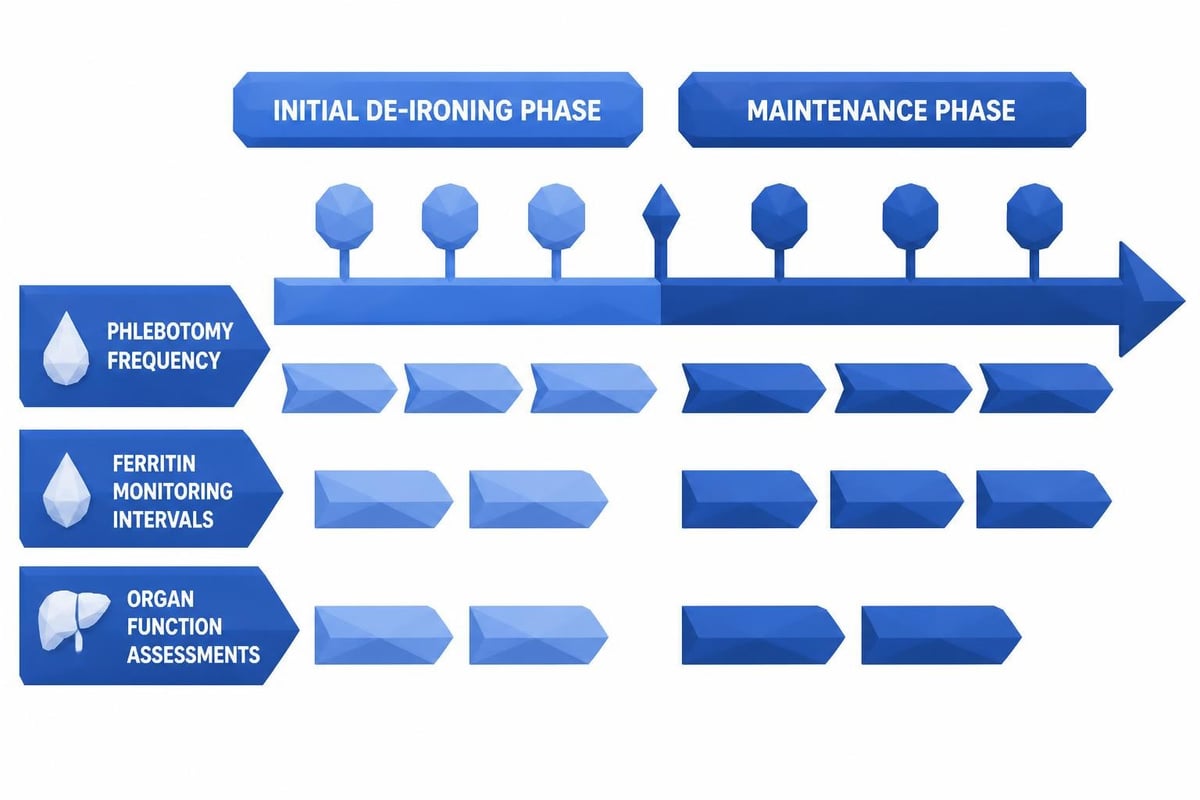
Phlebotomy Protocol
Initial de-ironing phase:
- Weekly or biweekly blood removal (typically 500 mL)
- Continue until ferritin reaches 50-100 ng/mL
- May require 6-24 months depending on initial iron burden
Maintenance phase:
- Phlebotomy every 2-4 months
- Target ferritin 50-100 ng/mL
- Frequency adjusted based on monitoring
Blood donation programs often cannot accept hemochromatosis patients due to regulatory restrictions, requiring dedicated therapeutic phlebotomy through medical facilities. However, some regions allow supervised donation after consultation with blood banks.
Monitoring Requirements
Regular testing ensures treatment adequacy and prevents both iron depletion and reaccumulation. Best practices for managing hereditary hemochromatosis recommend checking ferritin and transferrin saturation before each phlebotomy initially, then every 3-6 months during maintenance.
Complete blood counts monitor for anemia development. Liver enzymes, glucose, and cardiac function assessments detect organ damage and guide treatment intensity.
Convenient access to lab testing supports effective monitoring. Services like ordering labs without a doctor enable patients to track their iron levels between specialist visits, facilitating timely treatment adjustments.
Family Screening and Genetic Counseling
Hereditary hemochromatosis follows autosomal recessive inheritance for most forms, meaning two mutated gene copies must be present for disease manifestation. When someone receives a hemochromatosis diagnosis, family screening becomes important.
First-degree relatives (parents, siblings, children) have 25% probability of sharing both mutations if parents are carriers. Even siblings who test negative for mutations can be carriers, making cascade screening valuable for family planning.
The genetics of hereditary hemochromatosis involve complex penetrance patterns. Not everyone with homozygous C282Y mutations develops clinically significant iron overload. Penetrance estimates suggest 13-70% of C282Y homozygotes develop elevated ferritin, with fewer experiencing symptoms.
Genetic Testing Considerations
- Screen all first-degree relatives of diagnosed individuals
- Test children when both parents carry mutations
- Consider genetic testing before marriage in affected families
- Evaluate partners of known carriers for family planning
Affordable, accessible testing helps families understand their risk. Comparing lab testing options allows individuals to obtain genetic screening and iron panels without insurance barriers.
Lifestyle Modifications and Dietary Considerations
While phlebotomy remains the cornerstone treatment, dietary modifications support iron management in hereditary hemochromatosis. However, recommendations differ significantly from those for metabolic hyperferritinaemia.
For genetic hemochromatosis:
- Limit vitamin C supplements (increases iron absorption)
- Avoid iron-fortified foods when possible
- Moderate red meat consumption
- Avoid raw shellfish (infection risk with iron overload)
- Limit or avoid alcohol (reduces liver damage risk)
Tea consumption with meals may slightly reduce iron absorption due to tannin content, though this provides minimal benefit compared to phlebotomy. Calcium supplementation might decrease iron absorption, but evidence remains limited.
For metabolic hyperferritinaemia:
- Focus on metabolic syndrome management
- Weight reduction if overweight
- Exercise regularly
- Improve insulin sensitivity through diet
- Address fatty liver disease
Understanding which condition drives ferritin elevation guides appropriate interventions. Unnecessary dietary iron restriction in metabolic hyperferritinaemia provides little benefit while potentially causing nutritional deficiencies.
The Role of Accessible Lab Testing
Regular monitoring forms the foundation of effective hemochromatosis management. Traditional healthcare systems sometimes create barriers to frequent testing through referral requirements, insurance authorization delays, and appointment scheduling challenges.
Direct access to lab testing addresses these obstacles. Patients managing high ferritin genetic iron TIBC abnormalities benefit from convenient monitoring options that provide quick results without physician orders. Understanding lab results empowers patients to track their progress and communicate effectively with healthcare providers.
Transparent pricing eliminates surprise bills and allows better budgeting for chronic condition management. When monitoring requires quarterly or more frequent testing, knowing exact costs enables financial planning.
Emerging Research and Future Directions
Scientific understanding of genetic iron regulation continues evolving. Recent research explores the relationship between iron metabolism, inflammation, and metabolic disease, revealing complex interactions beyond simple iron overload.
Hepcidin-targeted therapies represent an active research area. Rather than removing iron through phlebotomy, future treatments might restore normal hepcidin function, preventing excessive absorption at its source. Several pharmaceutical companies are developing hepcidin analogs and regulators.
Gene therapy approaches for severe forms like juvenile hemochromatosis show promise in early studies. Correcting the underlying genetic defect could eliminate the need for lifelong phlebotomy in some patients.
Improved understanding of genetic modifiers helps explain why identical mutations produce varying clinical severity. Genome-wide association studies identify additional genes influencing iron metabolism, inflammation, and organ damage susceptibility.
Precision medicine approaches may eventually tailor monitoring and treatment intensity based on individual genetic profiles rather than universal protocols. Some C282Y homozygotes require aggressive treatment, while others need minimal intervention despite identical mutations.
Special Populations and Unique Considerations
Pregnancy complicates hereditary hemochromatosis management. Iron demands increase substantially during gestation, often temporarily resolving iron overload without intervention. However, women with hemochromatosis require careful monitoring to balance maternal needs with preventing excessive accumulation.
Children diagnosed through family screening rarely require treatment before puberty. Iron accumulation accelerates in males after adolescence and in females after menopause. Early diagnosis allows preventive monitoring before iron reaches damaging levels.
Elderly individuals newly diagnosed with high ferritin genetic iron TIBC patterns require different considerations. Phlebotomy tolerance decreases with age, and cardiovascular risks may limit aggressive de-ironing. Gentler protocols with smaller volumes or longer intervals between treatments may be appropriate.
Individuals with concurrent conditions affecting blood counts need specialized approaches. Anemia from other causes, polycythemia vera, or chronic kidney disease complicate standard phlebotomy protocols, requiring coordination between specialists.
Recognizing the connection between high ferritin genetic iron TIBC measurements and hereditary hemochromatosis enables early intervention before irreversible organ damage occurs. Systematic evaluation distinguishes genetic iron overload from secondary causes, guiding appropriate treatment through therapeutic phlebotomy and regular monitoring. Whether you need initial screening for suspected iron overload or ongoing monitoring to track treatment progress, Justlabs provides convenient access to comprehensive iron panels with transparent pricing and results delivered within 1-3 days, supporting effective management of genetic iron disorders.