Understanding your reproductive health starts with knowing your ovarian reserve, and Anti-Müllerian Hormone (AMH) testing has become the gold standard for assessing fertility potential. The relationship between AMH ovarian reserve by age reveals crucial insights about egg quantity and reproductive timeline. Whether you're planning for future family building, considering egg freezing, or simply want to understand your fertility status, AMH testing provides valuable data that changes significantly throughout your life.
What AMH Reveals About Ovarian Reserve
Anti-Müllerian Hormone is produced by small follicles in the ovaries, making it a direct indicator of the number of eggs remaining. Unlike other fertility markers that fluctuate throughout your menstrual cycle, AMH levels remain relatively stable month to month, providing a consistent measure of ovarian reserve.
AMH serves multiple clinical purposes:
- Predicting response to fertility treatments
- Assessing egg freezing candidacy
- Estimating time until menopause
- Evaluating ovarian function after medical treatments
- Understanding reproductive aging patterns
The hormone is measured through a simple blood test that can be performed at any time during your cycle. Understanding ovarian reserve measures helps healthcare providers and patients make informed decisions about reproductive planning and treatment options.
How AMH Testing Works
Modern AMH testing requires only a single blood draw, making it accessible and convenient for women seeking fertility information. The test measures the concentration of AMH in nanograms per milliliter (ng/mL) or picomoles per liter (pmol/L), depending on the laboratory standard used.
Results typically become available within a few days, and many women choose labs without insurance to access transparent pricing and faster turnaround times. This direct-access approach eliminates the need for insurance authorization and lengthy appointment scheduling.
AMH Ovarian Reserve by Age: Expected Ranges
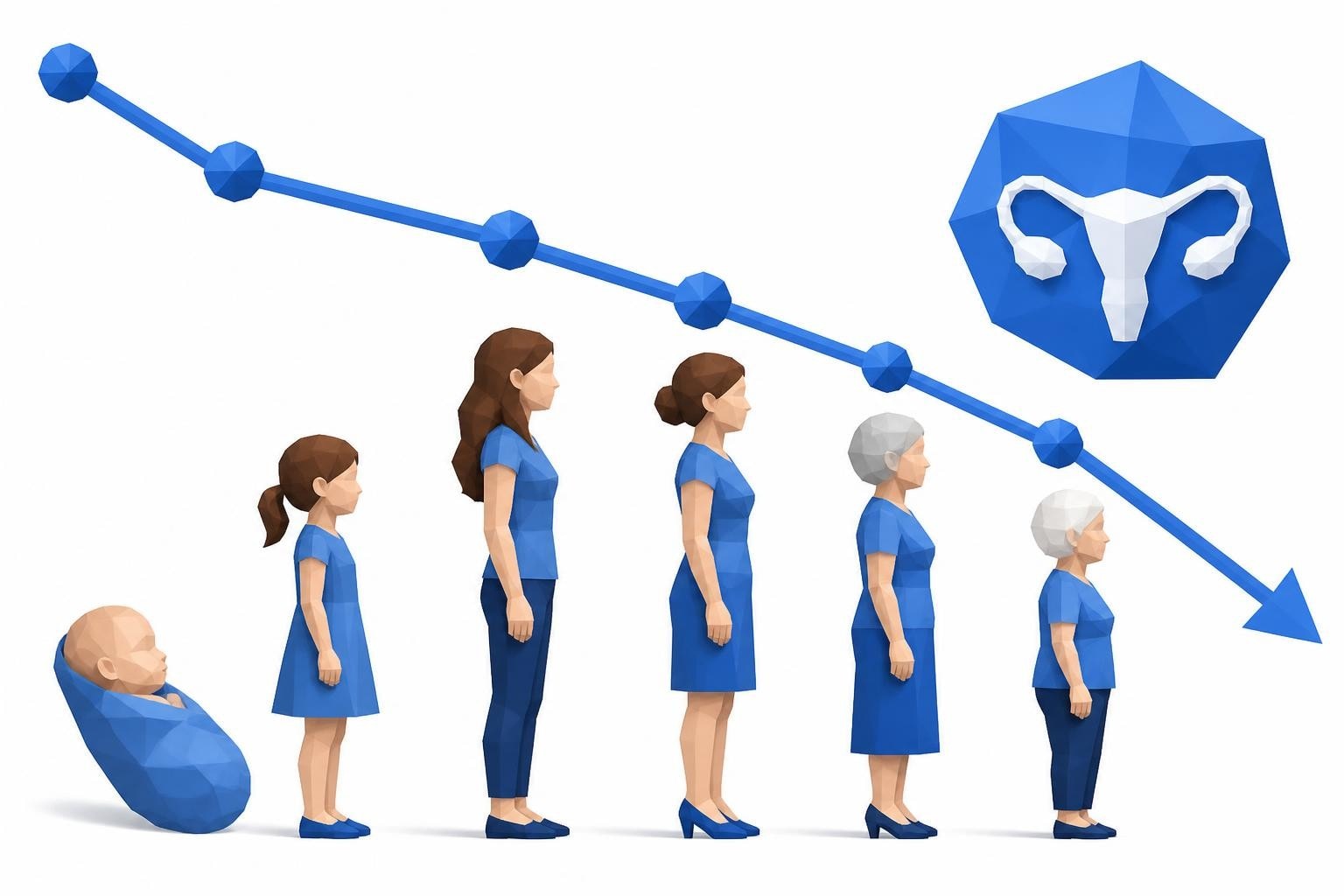
The relationship between AMH ovarian reserve by age follows a predictable decline from birth through menopause. Understanding these age-specific ranges helps contextualize individual results and set realistic expectations for fertility potential.
| Age Range | Average AMH (ng/mL) | Ovarian Reserve Status |
|---|---|---|
| Under 25 | 3.0 - 6.0 | High |
| 25-30 | 2.5 - 5.0 | Good |
| 30-35 | 1.5 - 4.0 | Adequate |
| 35-40 | 1.0 - 2.5 | Diminishing |
| 40-45 | 0.5 - 1.5 | Low |
| Over 45 | Below 0.5 | Very Low |
These ranges represent population averages, and individual variation is common. Research on AMH levels from conception to menopause demonstrates that AMH peaks in the mid-twenties and declines progressively afterward, with the rate of decline accelerating after age 35.
Peak Fertility Years
Women in their twenties typically show the highest AMH levels, reflecting maximum ovarian reserve. During this period, AMH ovarian reserve by age demonstrates optimal egg quantity and quality, corresponding with peak natural fertility rates.
The biological reality shows that fertility potential begins declining in the early thirties, with more significant decreases after 35. This decline reflects both decreasing egg quantity (measured by AMH) and diminishing egg quality (which AMH cannot measure directly).
The Thirties Transition
Between ages 30 and 35, most women experience moderate AMH decline while maintaining reasonable ovarian reserve. This five-year window represents a critical decision-making period for many regarding family planning and fertility preservation.
Key considerations during this phase:
- AMH levels begin showing more individual variation
- Fertility treatments may become more relevant
- Egg freezing remains highly effective
- Natural conception rates start declining gradually
By age 35, the acceleration of follicle depletion becomes more pronounced, making AMH testing particularly valuable for reproductive planning.
Interpreting Your AMH Results
Raw AMH numbers require context to become actionable information. The same AMH level may have different implications depending on your age, reproductive goals, and overall health status.
High AMH Levels
AMH levels above expected age-adjusted ranges may indicate abundant ovarian reserve, which generally represents good fertility potential. However, very high AMH (above 5.0 ng/mL) can also signal polycystic ovary syndrome (PCOS), a condition affecting hormone balance and ovulation.
Women with high AMH considering fertility treatments may be at increased risk for ovarian hyperstimulation syndrome (OHSS), requiring careful protocol adjustments.
Normal AMH Levels
Normal age-appropriate AMH levels suggest adequate ovarian reserve for your stage of life. Comprehensive information about AMH levels confirms that normal ranges vary considerably by age, making personalized interpretation essential.
Normal results provide reassurance but don't guarantee fertility, as AMH measures quantity rather than egg quality or other fertility factors like tubal patency or uterine health.

Low AMH Levels
Low AMH for your age indicates diminished ovarian reserve, which may affect both natural conception chances and fertility treatment outcomes. Understanding diminished ovarian reserve helps patients and providers develop appropriate reproductive strategies.
Low AMH doesn't mean:
- You cannot get pregnant naturally
- Fertility treatments won't work
- Your eggs are poor quality
- Menopause is imminent
It does suggest that time may be a more critical factor in your fertility planning, and proactive steps could be beneficial.
Factors Beyond Age Affecting AMH
While the connection between AMH ovarian reserve by age is strong, other factors influence individual levels and create variation from expected norms.
Hormonal contraceptives can suppress AMH levels by 20-30%, though the ovarian reserve itself remains unchanged. Testing should ideally occur after discontinuing hormonal birth control for several months, though this isn't always practical or necessary.
Medical Conditions and Treatments
Several health conditions impact AMH independently of age:
- Polycystic ovary syndrome typically elevates AMH levels
- Endometriosis may reduce AMH in some cases
- Autoimmune disorders can affect ovarian function
- Chemotherapy and radiation often cause dramatic AMH decline
- Ovarian surgery reduces follicle count and AMH
Vitamin D deficiency, obesity, and smoking have all been associated with lower AMH levels in research studies, though the mechanisms and significance remain under investigation.
Genetic and Ethnic Variations
Research on ovarian reserve modeling reveals that genetic factors contribute to the natural variation in AMH levels between individuals of the same age. Some women naturally have higher or lower reserves based on inherited traits.
Ethnic background also influences AMH levels, with studies showing differences in average levels between racial and ethnic groups independent of age or other factors.
Testing Strategies and Timing
Determining when to test AMH ovarian reserve by age depends on individual circumstances, reproductive goals, and risk factors for diminished reserve.
| Scenario | Recommended Testing Age | Frequency |
|---|---|---|
| Family history of early menopause | Age 25-28 | Every 2-3 years |
| Planning to delay childbearing | By age 30 | Baseline, then as needed |
| Fertility concerns or difficulty conceiving | Any age | Initial evaluation |
| Before/after cancer treatment | Before treatment, 6-12 months after | As medically indicated |
| Considering egg freezing | Age 28-35 | Before procedure |
Many women benefit from establishing a baseline AMH measurement in their late twenties or early thirties, then retesting if circumstances or goals change. Direct access to order labs without a doctor makes this proactive approach more feasible for informed reproductive planning.
Combining AMH with Other Tests
AMH provides one piece of the fertility puzzle but works best alongside complementary assessments. Antral follicle count (AFC) via ultrasound, follicle-stimulating hormone (FSH), and estradiol levels on cycle day 3 offer additional ovarian reserve information.
A comprehensive fertility evaluation also includes partner semen analysis, ovulation tracking, and anatomical assessment through ultrasound or hysterosalpingography.

AMH and Fertility Treatment Decisions
Understanding AMH ovarian reserve by age directly influences fertility treatment protocols and success predictions. Reproductive endocrinologists use AMH levels to customize medication dosages and set realistic expectations.
Treatment implications of different AMH levels:
- High AMH (>3.5 ng/mL): Lower medication doses to prevent overstimulation, excellent egg freezing candidate
- Normal AMH (1.0-3.5 ng/mL): Standard protocols typically effective, good treatment prognosis
- Low AMH (<1.0 ng/mL): Higher medication doses may be needed, more cycles might be required, consider donor options
Women with low AMH can still achieve pregnancy through IVF, though they may produce fewer eggs per cycle and require multiple treatment cycles.
Egg Freezing Considerations
AMH testing is particularly crucial for women considering elective egg freezing for fertility preservation. Higher AMH levels generally predict better egg yield from freezing cycles, making the investment more efficient.
The ideal age window for egg freezing is typically 30-37, balancing reasonable AMH levels with good egg quality. Women with lower AMH may need multiple freezing cycles to bank adequate eggs for future family building.
Limitations of AMH Testing
Despite its value, AMH ovarian reserve by age has important limitations that prevent it from being a complete fertility measure.
AMH cannot assess egg quality, which declines significantly with age regardless of quantity. A 40-year-old woman with high AMH still faces age-related egg quality challenges that affect conception rates and miscarriage risk.
The test also doesn't evaluate other crucial fertility factors like tubal function, uterine receptivity, or partner sperm quality. The role of AMH in assessing ovarian function emphasizes that AMH represents one component of comprehensive fertility evaluation.
Test Variability and Accuracy
Different laboratories use various AMH testing platforms that can produce slightly different results for the same sample. Knowing your laboratory's specific reference ranges and testing methodology is essential for accurate interpretation.
Single AMH measurements provide a snapshot but don't capture individual trajectories. Some women experience faster decline than others, making serial testing over time more informative than isolated values.
Proactive Reproductive Planning
Knowledge of AMH ovarian reserve by age empowers informed decision-making about reproductive timing and options. Early testing allows women to make choices aligned with their personal and professional goals.
For those with normal or high AMH who wish to delay childbearing, regular monitoring helps track changes and signal when action might become necessary. This proactive approach reduces the anxiety of uncertainty while maintaining reproductive options.
Women discovering low AMH gain valuable information that can accelerate family-building timelines, prompt fertility treatment consultation, or initiate egg freezing while viable options remain.
Financial Accessibility of Testing
The cost of AMH testing varies significantly depending on whether you use insurance or self-pay options. Traditional healthcare routes may require doctor appointments, insurance authorization, and copays that increase overall expense and delay results.
Transparent lab test pricing through direct-access services eliminates surprise costs and reduces the barrier to obtaining this important health information. Many women find self-pay AMH testing more affordable and convenient than navigating traditional healthcare channels.
Age-Specific Recommendations
The relationship between AMH ovarian reserve by age suggests different action items for various life stages.
Women Under 30
If you have no fertility concerns or family history of early menopause, routine AMH testing isn't typically necessary. However, baseline testing can provide valuable information if you're planning significant reproductive delay or want comprehensive health data.
Consider testing if you have irregular periods, PCOS symptoms, or have undergone treatments that might affect ovarian function.
Women 30-35
This age range represents an optimal time for baseline AMH assessment, particularly if you haven't yet started trying to conceive or plan to wait several more years. Results can inform decisions about timing and whether proactive measures like egg freezing make sense.
Annual or biannual testing during this window helps track your individual trajectory and identify accelerated decline requiring action.
Women 35-40
AMH testing becomes increasingly relevant after 35, as both quantity and quality decline accelerate. If you're actively trying to conceive, AMH results help determine whether fertility treatment consultation is warranted.
For those not yet trying, AMH provides crucial information about remaining fertility window and urgency of decision-making.
Women Over 40
After 40, AMH ovarian reserve by age typically shows low levels, but testing remains valuable for fertility treatment planning and determining realistic options. Very low AMH may indicate that donor eggs represent the best path to pregnancy.
Testing can also help predict menopausal timing for women experiencing irregular cycles or perimenopausal symptoms.
Beyond the Numbers
While understanding AMH ovarian reserve by age provides valuable quantitative data, fertility represents a complex interplay of biological, psychological, and social factors. AMH levels inform but don't determine your reproductive story.
Many women with low AMH conceive naturally, while some with excellent AMH face other fertility challenges. The test serves as one tool among many for understanding reproductive health and making informed choices.
Emotional responses to AMH results are valid and common, whether relief, concern, or urgency. Processing results with healthcare providers, fertility specialists, or counselors helps translate numbers into personalized action plans.
Making AMH Testing Accessible
Access to convenient, affordable AMH testing continues expanding as women seek proactive health information. Modern platforms now offer streamlined processes from ordering through results delivery.
The traditional model requiring doctor visits, insurance navigation, and extended wait times has given way to direct-access options that respect women's time and autonomy. How modern lab testing works demonstrates the simplified process making fertility information more accessible than ever.
Quick turnaround times mean results arrive within days rather than weeks, allowing timely decision-making when reproductive planning requires current data. Digital result delivery provides privacy and convenience while maintaining medical-grade accuracy.
Understanding AMH ovarian reserve by age gives you powerful insights into your reproductive timeline and helps inform important life decisions. Whether you're planning ahead, addressing current fertility concerns, or simply want comprehensive health information, AMH testing provides actionable data about your ovarian reserve. Justlabs makes accessing this important testing simple and affordable, with transparent pricing and results delivered in 1-3 days, so you can take charge of your reproductive health without the complexity of traditional healthcare navigation.