Prostate-specific antigen (PSA) testing has become a cornerstone of prostate health monitoring, but elevated total PSA levels alone don't always indicate cancer. The free vs total PSA ratio provides crucial context that helps physicians distinguish between benign prostate conditions and potentially cancerous growths, ultimately reducing the number of unnecessary biopsies performed each year. This ratio calculation has revolutionized how healthcare providers approach prostate cancer screening, offering a more nuanced understanding of what elevated PSA levels actually mean for patient health.
Understanding PSA and Its Forms in the Bloodstream
Prostate-specific antigen is a protein produced by cells in the prostate gland. When released into the bloodstream, PSA exists in two primary forms: free PSA, which circulates unbound to other proteins, and complexed PSA, which attaches to other blood proteins. Together, these two forms constitute total PSA, the measurement most commonly referenced in routine screening.
The distinction between these forms matters significantly. Benign prostatic hyperplasia (BPH) and prostatitis tend to produce more free PSA, while prostate cancer cells typically generate more complexed PSA. This fundamental biological difference forms the basis for why the free vs total PSA ratio serves as such a valuable diagnostic tool.
How the Ratio Calculation Works
Healthcare providers calculate the free vs total PSA ratio by dividing free PSA by total PSA and multiplying by 100 to get a percentage. For example, if a patient has 1.0 ng/mL of free PSA and 4.0 ng/mL of total PSA, the ratio would be 25%. This straightforward calculation provides immediate clinical insight.
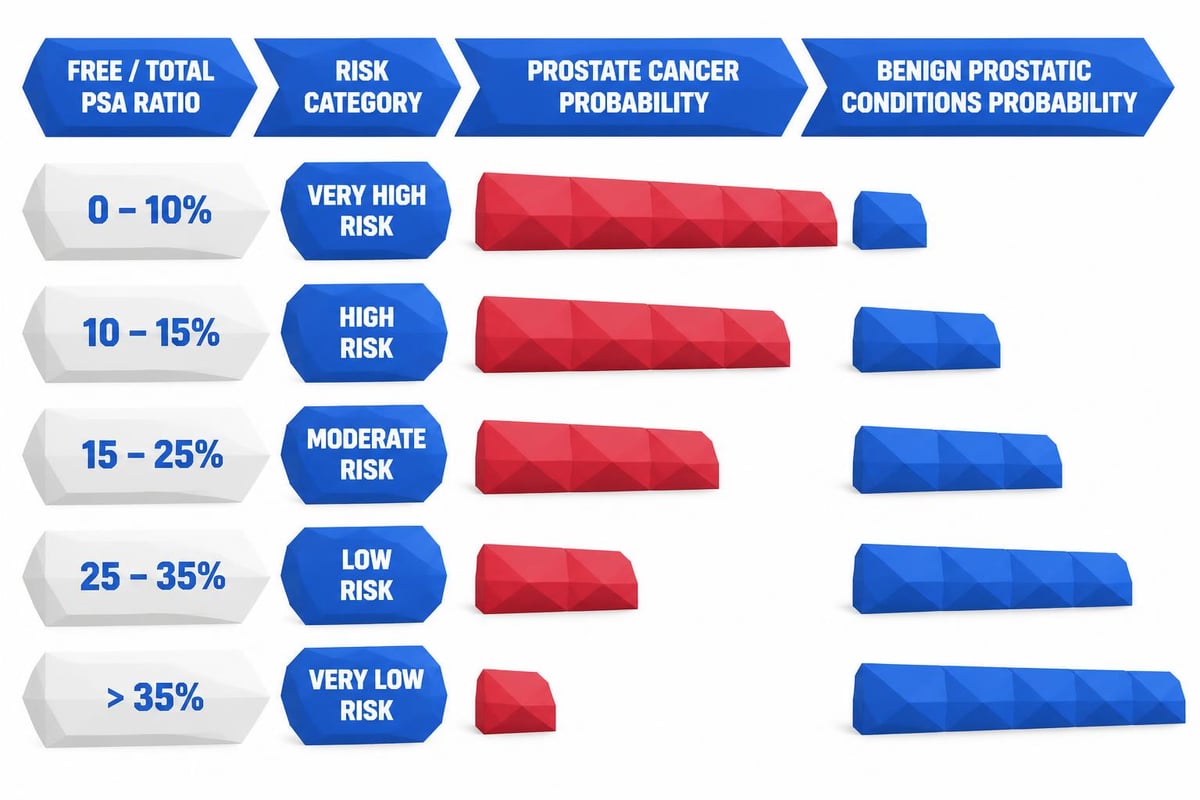
Key ratio thresholds typically used:
- Above 25%: Generally suggests benign conditions are more likely
- 15% to 25%: Intermediate risk zone requiring careful evaluation
- Below 15%: Higher suspicion for prostate cancer, biopsy often recommended
- Below 10%: Significantly elevated cancer risk
These cutoffs aren't absolute rules but rather guidelines that physicians use alongside other clinical factors, including patient age, prostate size, and family history.
When Testing the Free vs Total PSA Ratio Makes Clinical Sense
Not every patient with an elevated PSA reading requires ratio testing. Understanding when this test provides value helps optimize its diagnostic utility while controlling healthcare costs.
The free vs total PSA ratio proves most valuable when total PSA falls within the "gray zone" of 4 to 10 ng/mL. In this range, total PSA elevation could indicate either cancer or benign conditions, making additional context essential for decision-making. Below 4 ng/mL, cancer risk remains relatively low, while above 10 ng/mL, biopsy is typically recommended regardless of ratio results.
Specific Clinical Scenarios
Several patient situations warrant ratio testing consideration:
- First-time elevated PSA: When initial screening shows PSA between 4-10 ng/mL in asymptomatic men
- Monitoring known BPH: Tracking changes in patients with diagnosed benign prostatic hyperplasia
- Post-treatment surveillance: Following patients after prostate cancer treatment for recurrence signs
- Family history concerns: Men with first-degree relatives who had prostate cancer
- Age-specific elevations: Younger men (under 60) with borderline PSA levels
Direct-to-consumer lab services now make it easier than ever to access these tests without insurance barriers, empowering patients to take proactive control of their prostate health monitoring.
How the Ratio Reduces Unnecessary Biopsies
The primary clinical benefit of the free vs total PSA ratio lies in its ability to prevent unnecessary invasive procedures. Before ratio testing became standard practice, many men with elevated total PSA underwent biopsies that ultimately revealed benign conditions, exposing them to procedural risks without clinical benefit.
Studies have demonstrated that incorporating ratio analysis into prostate cancer screening protocols can reduce unnecessary biopsies by 20-30% while maintaining high cancer detection rates. This represents significant value for both patients and the healthcare system.
| PSA Scenario | Without Ratio Testing | With Ratio Testing |
|---|---|---|
| Total PSA 6.5 ng/mL | Biopsy recommended | Ratio checked first |
| Ratio >25% | Would undergo biopsy | Biopsy often avoided |
| Ratio <15% | Would undergo biopsy | Biopsy recommended |
| Outcome | More unnecessary procedures | Targeted biopsies only |
The ratio's predictive value proves particularly important for men who experience anxiety about biopsy procedures or those with medical conditions that increase procedural complications risk.
Risk Stratification Benefits
Beyond simple biopsy avoidance, the free vs total PSA ratio enables more sophisticated risk stratification. This approach allows physicians to differentiate between patients who need immediate intervention and those who can safely pursue active surveillance.
Men with intermediate-risk ratios (15-25%) might undergo additional testing, such as prostate MRI or newer biomarker panels, before deciding on biopsy. This tiered approach optimizes diagnostic accuracy while minimizing patient burden.
Interpreting Your Test Results Accurately
Understanding free vs total PSA ratio results requires context beyond the numbers themselves. Several factors influence PSA levels and ratio calculations, making interpretation more complex than simply comparing your result to reference ranges.
Factors that can affect PSA measurements:
- Recent sexual activity or ejaculation
- Prostate manipulation during digital rectal exam
- Urinary tract infections or prostatitis
- Certain medications, particularly finasteride or dutasteride
- Vigorous exercise, especially cycling
- Recent urological procedures
For the most accurate results, patients should avoid ejaculation for 48 hours before testing, inform their healthcare provider about all medications, and ensure adequate recovery time from any recent prostate procedures. Many patients who order labs without a doctor's referral appreciate having control over testing timing to optimize these pre-test conditions.
Age-Adjusted Considerations
PSA levels naturally increase with age as the prostate enlarges. A total PSA of 4.0 ng/mL carries different implications for a 45-year-old versus a 70-year-old man. Similarly, the free vs total PSA ratio should be interpreted within age-appropriate contexts.
| Age Range | Median Total PSA | Concern Threshold | Typical Free % |
|---|---|---|---|
| 40-49 years | 0.7 ng/mL | >2.5 ng/mL | 25-30% |
| 50-59 years | 1.0 ng/mL | >3.5 ng/mL | 22-27% |
| 60-69 years | 1.4 ng/mL | >4.5 ng/mL | 20-25% |
| 70-79 years | 2.0 ng/mL | >6.5 ng/mL | 18-23% |
These age-specific reference points help both patients and providers understand whether test results fall within expected ranges or warrant further investigation.
Limitations and Complementary Testing Approaches
While the free vs total PSA ratio provides valuable diagnostic information, it has limitations that patients should understand. The ratio doesn't definitively diagnose or rule out prostate cancer; it simply refines probability estimates to guide clinical decision-making.
Research shows that the ratio's predictive accuracy varies depending on the total PSA level and individual patient characteristics. In some populations, particularly men with very low or very high total PSA levels, the ratio adds minimal additional diagnostic value.
When Additional Testing Is Warranted
Patients with concerning ratio results or unclear clinical pictures may benefit from complementary diagnostic approaches:
- Prostate Health Index (PHI): Combines total PSA, free PSA, and [-2]proPSA for enhanced accuracy
- 4Kscore Test: Uses four kallikrein markers to calculate cancer probability
- Multiparametric MRI: Imaging that identifies suspicious areas before biopsy
- PCA3 Urine Test: Measures a gene expressed primarily in prostate cancer cells
- Biomarker panels: Various combinations of proteins and genetic markers
The availability of transparent lab test pricing makes it easier for patients to understand the cost implications of pursuing multiple complementary tests when building a comprehensive diagnostic picture.
Practical Steps for Prostate Health Monitoring
Men concerned about prostate health should approach screening systematically, starting with baseline total PSA testing in their 40s or 50s, depending on risk factors. Establishing baseline values enables more meaningful interpretation of future changes.
If total PSA comes back elevated, particularly in the 4-10 ng/mL range, the free vs total PSA ratio becomes the logical next step. Rather than immediately proceeding to biopsy, this intermediate testing stage provides critical risk stratification information.
Creating Your Monitoring Schedule
Recommended testing frequency depends on individual risk profiles and previous results:
- Low risk with normal PSA: Every 2-4 years after age 50
- Moderate risk or borderline PSA: Annually
- High risk or elevated ratio: Every 6 months with physician consultation
- Known BPH: As recommended by urologist, typically annually
Maintaining consistent testing schedules allows for trend analysis, which often provides more insight than single time-point measurements. Understanding how lab testing works helps patients stay on track with their monitoring schedules without the friction of scheduling doctor appointments for each test order.
Cost Considerations and Access to Testing
Traditional prostate screening through insurance often involves copays, deductibles, and the requirement for physician referrals, creating barriers that delay necessary testing. The total cost of PSA testing through conventional channels can range from $30 to over $200 depending on insurance coverage.
Free vs total PSA ratio testing historically required separate orders and additional physician visits, compounding both time and cost burdens. Modern self-pay lab services have changed this equation significantly, offering bundled PSA testing panels at transparent, upfront prices typically lower than insurance-based testing for many patients.
Comparing testing approaches:
| Aspect | Traditional Route | Self-Pay Lab Testing |
|---|---|---|
| Physician visit required | Yes, before testing | No |
| Insurance verification | Required | Not applicable |
| Price transparency | Variable, uncertain | Fixed, upfront |
| Results timeline | 3-7 days | 1-3 days |
| Schedule flexibility | Limited by appointments | Order anytime online |
Many patients find that self-pay testing through services offering accessible lab testing options provides greater convenience and often comparable or lower costs than navigating insurance channels.
The Role of Patient Empowerment in Screening Decisions
Modern healthcare increasingly recognizes the value of informed patients participating actively in their health decisions. Understanding the free vs total PSA ratio empowers men to engage in meaningful conversations with their healthcare providers about screening strategies and intervention thresholds.
Patients who educate themselves about PSA testing nuances often experience less anxiety about borderline results because they understand the additional context that ratio testing provides. This knowledge helps when reviewing lab results and deciding on appropriate next steps with medical guidance.
Questions to Ask Your Healthcare Provider
Armed with ratio test results, patients should prepare specific questions for their physician consultations:
- How does my ratio compare to typical values for my age and risk profile?
- Given my ratio, what's the estimated probability of cancer versus benign conditions?
- Should we pursue additional biomarker testing before considering biopsy?
- How frequently should I retest to monitor for changes?
- What lifestyle modifications might help optimize my prostate health?
These focused questions facilitate productive clinical discussions that lead to personalized screening strategies rather than one-size-fits-all protocols.
Future Directions in Prostate Cancer Screening
The free vs total PSA ratio represents just one advancement in the evolving landscape of prostate cancer detection. Emerging technologies promise even greater diagnostic precision, potentially further reducing unnecessary biopsies while improving early cancer detection.
Artificial intelligence algorithms now analyze combinations of biomarkers, imaging findings, and clinical variables to generate highly personalized risk scores. These tools may eventually integrate ratio data with genetic markers, prostatic volume measurements, and family history into comprehensive risk calculators.
Promising developments on the horizon:
- Liquid biopsy techniques detecting circulating tumor DNA
- Advanced imaging modalities identifying aggressive cancers specifically
- Genetic risk profiling based on inherited variants
- Urinary biomarkers measured from simple at-home collections
- Machine learning models predicting cancer aggressiveness
Despite these innovations, the free vs total PSA ratio will likely remain relevant as a cost-effective, accessible screening tool that provides substantial clinical value for the majority of patients undergoing prostate health monitoring.
Understanding the free vs total PSA ratio helps men make informed decisions about prostate health screening while potentially avoiding unnecessary invasive procedures. This simple calculation provides critical context for elevated PSA levels, distinguishing between cancer risk and benign conditions. When you need convenient access to PSA testing with transparent pricing and quick results, Justlabs offers self-pay lab testing services that put you in control of your health monitoring without insurance hassles or required doctor visits.